LONG COVID: IMMUNOGENETIC MARKERS ASSOCIATED WITH PROGRESSION
REGISTRO DOI:10.5281/zenodo.11371278
Antonio Ariel Rodrigues Saraiva1
Daniella Matos Mendonça de Melo1
Ana Maisa Passos-Silva2,3,4,5
Adrhyan Araújo2,3,4
Deusilene Vieira 2,3,4,5
ABSTRACT
The SARS-CoV-2 virus, originating in Wuhan, China, in December 2019, triggered the COVID-19 pandemic, spreading globally through respiratory droplets and contact with contaminated surfaces. Characteristic symptoms include fever, dry cough and shortness of breath, usually appearing between the 2nd and 14th day after infection. However, COVID-19 can also develop into a chronic condition known as long COVID, in which symptoms persist for more than 4 weeks. In addition to conventional symptoms, such as fatigue, shortness of breath, muscle pain and cognitive problems, this syndrome can present a wide range of manifestations. The groups most susceptible to long COVID are those who have experienced a severe form of the disease, have not been vaccinated and/or have previous comorbidities. The pathophysiology of Post-COVID Syndrome is complex, involving target organ damage, inflammation, immune dysfunction, adverse drug effects and psychosocial issues. The sequelae can be diverse and long-lasting, negatively impacting patients’ quality of life. Despite efforts to better understand COVID-19 and its consequences, there are still significant gaps in knowledge, especially regarding post-COVID syndrome. Research into long COVID is ongoing, but more studies are needed to fully understand its natural course and develop effective treatment and management approaches. The global response to the pandemic continues to evolve as new information emerges and public health strategies are adapted to meet the challenges presented by the virus.
Key words: COVID-19, Long COVID, Chronic Manifestation, SARS-CoV-2, Symptoms.
BACKGROUND
In December 2019, in Wuhan, China, the disease caused by the SARS-CoV-2 virus, called Coronavirus Disease 2019 (COVID-19), spread rapidly due to the high transmissibility profile of the virus, through respiratory droplets and contact with contaminated people or objects (Da Silva et al., 2021).
To get an idea of the epidemiology of the disease, as of September 2022, there were 613,410,796 confirmed cases worldwide and 6,518,749 deaths from COVID-19. At national level, 34,638,288 cases have been confirmed in Brazil with 685,835 deaths (BRASIL. Ministério da Saúde, 2021;BRASIL. Ministério da Saúde, 2024).
As for the typical symptoms of the disease, the main ones are fever, dry cough and shortness of breath in the acute form, with the possibility of other associated symptoms and progression to the severe form (Gorbalenya et al., 2020; M. S. Han et al., 2021). Typical symptoms usually appear between the 2nd and 14th day of infection (Da Silva et al., 2021; Huang et al., 2020). However, when symptoms persist for more than 4 weeks after infection, long COVID is identified, which consists of a multisystemic condition of several symptoms in addition to the conventional ones, such as fatigue, shortness of breath, cough, chest pain, heart palpitations, fever, headache, muscle pain, gastrointestinal problems and loss of taste and smell, and can also involve psychological problems and cognitive symptoms, such as depression, anxiety, post-traumatic stress disorder (Da Silva et al., 2021;Gorbalenya et al., 2020).
The people most susceptible to long COVID are those who have suffered from a severe form of the disease, those who have not received the COVID-19 vaccine and those who already had comorbidities before becoming infected with the virus (Townsend et al., 2020). In addition, there are important immunogenetic markers that are associated with disease progression, such as ACE2 and TMPRSS2 (Fernández-de-las-Peñas et al., 2022; RESER, 2021).
Several factors can contribute to the establishment of long COVID, such as sequelae of target organ damage due to viral toxicity, hyper-inflammation of cellular tissues, deregulation of the autoimmune response, microvascular endothelial damage, hyper-coagulation, secondary infections, prolonged hospitalization, especially in the ICU (critically ill patients), decompensation of clinical comorbidities, adverse effects of medications used in treatment, post-traumatic stress and other psychological conditions, social and financial impact (SANTOS FILHO & LIMA, 2021;Gorbalenya et al., 2020)(Townsend et al., 2020).
Among these risk factors, it is important to highlight the sequelae, which can be distinct and wide-ranging, the main ones being fatigue, hyposmia and ageusia and headaches, which can persist indefinitely, generating functional impairment and negatively affecting patients’ quality of life (Costa Da Costa et al., 2023;Townsend et al., 2020).
Therefore, as COVID-19 is a recent disease, its natural course and consequences are still poorly understood, with few studies of the population affected by this post-COVID syndrome. Thus, the World Health Organization has defined post-COVID-19 as “occurring in individuals with a history of probable or confirmed SARS-CoV-2 infection, usually 3 months after the onset of COVID-19 with symptoms that last at least 2 months and cannot be explained by an alternative diagnosis”.
METHODS
DATA AND COLLECT METHOD
Searches were carried out on the CORONAVÍRUS BRASIL, PubMed and Google Scholar platforms in order to find subjects that were relevant to the topic. Thus, search terms related to COVID-19, Long COVID-19 Syndrome, epidemiology, pathology, symptomatology, virological aspects, genetic markers and diagnosis were used.
SELECTION OF BIBLIOGRAPHIC REFERENCES AND ELIGIBILITY CRITERIA
Cross-sectional, cohort and case-control studies from indexed journals were selected. This included research on the maintenance of symptoms following viral infections with SARS-CoV-19 and its strains in Brazil and around the world, assessing the pathogenicity, immunogenetics and epidemiology of the virus. In addition, studies were selected that address the diagnosis of post-COVID syndrome in order to verify the delimitation of the technique for this and the specificity of the symptomatology that characterizes it as signs and symptoms of the syndrome. In addition, articles and platforms explaining the development of viral pathology and its transmission were analyzed.
IDENTIFICATION OF STUDY SELECTION
Searches were carried out until March 2024, from which 42,400 citations were identified, of which 425 met the eligibility criteria and 32 were selected for evaluation of the full text. All the studies comprised observational research and all met the proposed inclusion criteria.
RESULTS E DISCUSSION
VIROLOGICAL ASPECTS
Belonging to the Coronaviridae family, Coronavirinae subfamily and Betacoronavirus genus, SARS-CoV-2 is an enveloped virus containing a single-stranded, positively polar RNA genome (Saadi et al., 2021). Their RNA has approximately 30,000 base pairs and is polyadenylated at the 3′ end and has a CAP at the 5′ end (Bárbara Chiocca Do Nascimento et al., 2020).
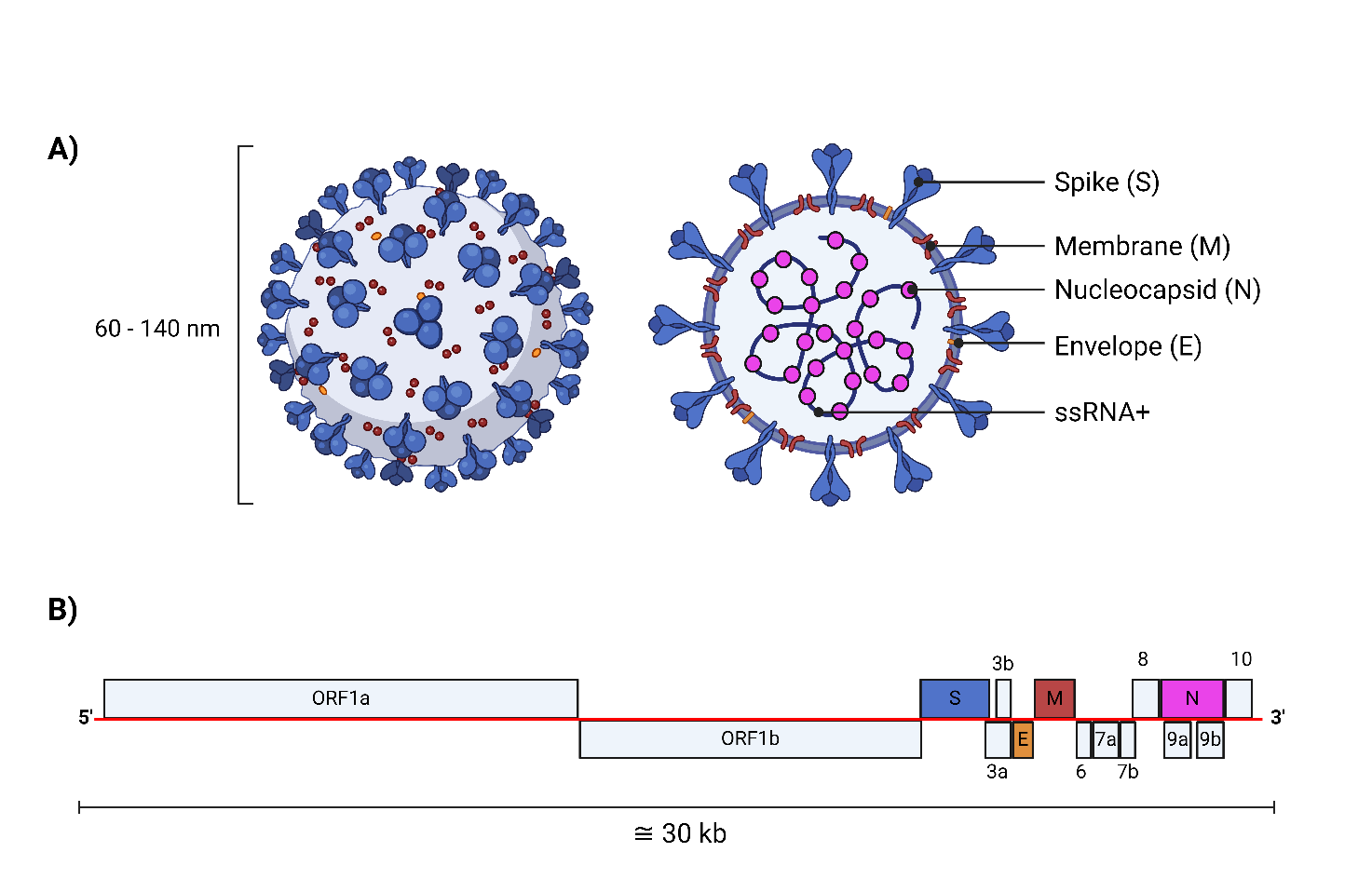
Figure 1 – Structural characteristics of the SARS-CoV-2 viral particle.
Subtitle: A) The SARS-CoV-2 viral particle is approximately 60 to 140 nm in size, in its structure the Spike, Membrane, Nucleocapsid and Envelope proteins are the structural proteins, and its genome is composed of an ssRNA+; B) Genomic organization of the viral genetic material (Created on BioRender.com).
From a structural point of view, there are two important aspects to highlight: Firstly, there is a high concentration of proteins in the lipid layer surrounding the virus (Zhirnov & Poyarkov, 2021). Structurally, 3 are present in this layer: the S glycoprotein (spike), the M protein (membrane) and the E protein (envelope) (Ramos et al., 2020). The S-glycoprotein is the most abundant and plays a crucial role in binding the virus to the host cell, thus initiating the fusion process between the viral envelope and the cell membrane, which is essential for the virus’s replicative cycle (Boson et al., 2021). This glycoprotein is made up of two subunits, S1 and S2, which become independent after cleavage by cellular proteases (Ramos et al., 2020; Reser, 2021). The functions of these subunits make them an important target for antibodies and inhibitor molecules (Saadi et al., 2021; M. Srivastava et al., 2021; Sun et al., 2021)
Secondly, the SARS-CoV-2 genome is remarkably long, at around 30 kilobases (kb), which is unusual for RNA viruses (Bárbara Chiocca Do Nascimento et al., 2020). This is due to the presence of a domain with 3′-5′-exoribonuclease activity, which is part of the protein complex involved in viral genome replication (Boson et al., 2021; Saadi et al., 2021). This activity makes it possible to correct transcription errors introduced naturally during the copying of the genomic RNA template by RNA-dependent RNA polymerase (Ramos et al., 2020). This ability to correct errors reduces the mutation rate of the virus, giving it a genomic stability that is unusual for RNA viruses and preventing an excess of mutations that could be damaging (Bárbara Chiocca Do Nascimento et al., 2020; Townsend et al., 2020).
SARS-CoV-2 infection begins with the interaction of the viral particle with the host cell (Cao et al., 2021). This process can occur through the inhalation of droplets containing the virus, originating from the respiratory secretions of an infected individual, or through the inoculation of viral particles present in these secretions, which contaminate hands or objects and are then transferred to the nose, mouth or eyes, thus allowing the virus access to the epithelial cells of the respiratory mucous membranes (Da Silva et al., 2021).
The incubation period for SARS-CoV-2 is generally short, on average 4 to 5 days after exposure to the virus (Da Silva et al., 2021). During this phase, the virus replicates in the epithelial cells lining the mucous membranes of the nose and throat, where they express the ACE2 receptor and the TMPRSS2 protease (Boson et al., 2021; Radzikowska et al., 2020). Unlike SARS-CoV-1, individuals infected with SARS-CoV-2 can transmit the virus before developing any symptoms, which contributes to its rapid spread (Z. Chen et al., 2022). In addition, SARS-CoV-2 has a propensity to accumulate in large concentrations in the nasal and throat mucous membranes, facilitating its transmission (Reser, 2021; Le Bert et al., 2020)
Finally, there is still uncertainty about how long the virus remains in the respiratory tract of an infected individual (Nunes et al., 2022). A recent study suggests that the presence of the virus can be detected for around 17 days from the onset of symptoms in diagnosed individuals (M. S. Han et al., 2021).
LONG COVID
Although there is still much uncertainty about how exactly prolonged COVID syndrome develops, it is clear that COVID-19 triggers a range of complications, involving everything from a severe respiratory infection to exacerbated immune responses and coagulation problems (Rojas et al., 2022). These complications, in turn, seem to be linked to a wide range of persistent symptoms, affecting various systems of the human body (Rojas et al., 2022; Shalev et al., 2017)
After a serious episode of infection or trauma, the human body reacts with an aggressive immune response, followed by a prolonged period of attempted anti-inflammatory regulation (Rojas et al., 2022; Shalev et al., 2017). This process, known as compensatory anti-inflammatory response syndrome, may be at the root of the prolonged manifestations seen after severe infections, such as COVID-19 (T. Yang et al., 2022). Long-term effects of SARS-CoV-2 infection include persistent fatigue, muscle pain, loss of appetite and lung damage (Al-Aly et al., 2021; Townsend et al., 2020).
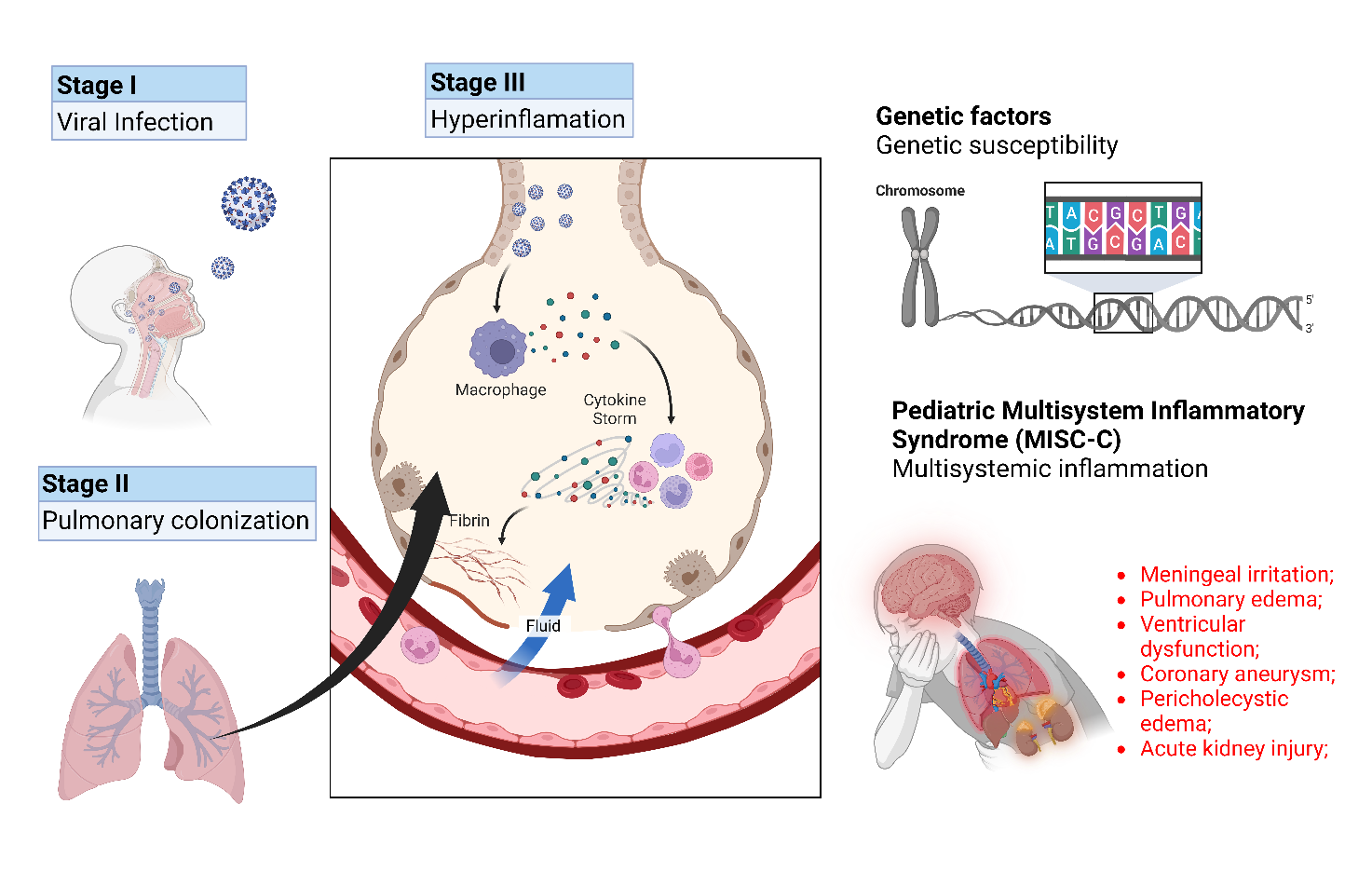
Figure 2: Stages of the pathophysiology of COVID-19 up to the severe manifestations resulting from hyperinflammation syndromes.
Subtitle: Phase I: Early SARS-CoV-2 infection, which can be asymptomatic or mildly symptomatic; Phase II –> The pulmonary phase, which is severe in adults but mild or absent in many children; Phase III –> Early infection triggers the activation of macrophages followed by the stimulation of T helper cells, which leads to the release of cytokines, the stimulation of macrophages, neutrophils and monocytes, along with the activation of B cells and plasma cells with the production of antibodies leading to a hyperimmune response.
Post-COVID syndrome presents a wide range of physical and mental symptoms, documented in more than 100 studies, which significantly impact quality of life, including the ability to work and socialize (Hou et al., 2020; Iqbal et al., 2021). Common symptoms include fatigue, memory problems, shortness of breath, depression, anxiety and joint pain. These symptoms mainly affect the respiratory, cardiovascular and nervous systems (Townsend et al., 2020; Xie & Al-Aly, 2022).
The diagnosis and treatment of post-COVID syndrome is challenging due to the diversity and overlap of symptoms, which can resemble other health conditions unrelated to COVID-19 (Boson et al., 2021; Meng et al., 2021). In addition, there is evidence suggesting a possible increase in the identification of autoimmune diseases in individuals after becoming infected with SARS-CoV-2, such as diabetes and rheumatoid arthritis (Rojas et al., 2022; Shah et al., 2020).
In addition to the heart, the pancreas and liver are frequently affected organs, especially in hospitalized patients (Al-Aly et al., 2021). Symptoms such as headache are common in patients with pancreatic inflammation. In addition, symptoms such as shortness of breath, chest pain and abdominal pain are seen in post-COVID syndrome (Ramos et al., 2020)Mental health impacts, such as anhedonia, lethargy, loss of appetite, insomnia and sadness, are also frequent among COVID-19 recoveries (Maglietta et al., 2022; T. Yang et al., 2022). Arthralgia is another common symptom and can mimic rheumatological disorders, as well as being associated with the side effects of certain drugs used to treat COVID-19 (Shah et al., 2020).
Figure 3 – Systemic damage and persistent symptoms commonly found in the long term with COVID-19.
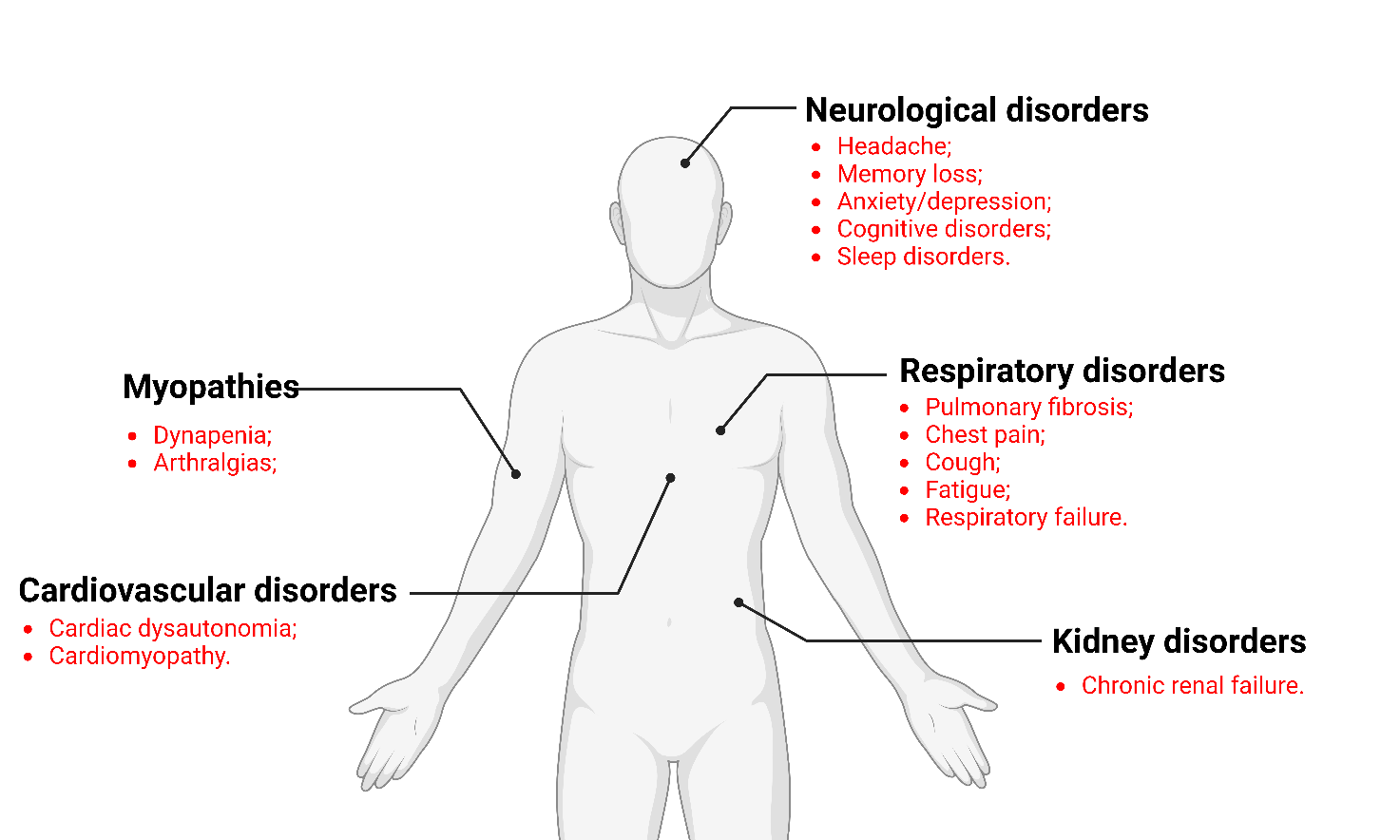
Subtitle: Post-COVID symptoms, such as fatigue, memory problems, shortness of breath and joint pain, impact various systems in the body, especially the respiratory, cardiovascular and nervous systems. The heart, pancreas and liver are often affected. Identifying and treating these symptoms is challenging due to the diversity and overlapping of manifestations, and they can be confused with other medical conditions (Created in BioRender.com).
Demographic factors and comorbidities are related to the persistence of post-COVID symptoms, while the severity of the disease is associated with a greater likelihood of persistent symptoms, probably due to the exacerbated immune response (Shah et al., 2020; Shalev et al., 2017). Effective recovery strategies are needed to help post-COVID patients return to normal life and cope with the associated psychological symptoms (Meng et al., 2021; T. Yang et al., 2022).
The largest cohort study to date, carried out by Al-Aly et al., 2021, included 73,435 participants and highlighted the persistence of a variety of symptoms after the first 30 days of SARS-CoV-2 infection, reinforcing the complexity and multisystemic nature of the post-COVID syndrome..
GENETIC MARKERS X LONG COVID
Several studies have been dedicated to studying the unique mechanisms of viral infection, pointing to a shared entry route with coronavirus-like viruses, suggesting the participation of the S1 receptor of the angiotensin-converting enzyme 2 (ACE2) and the transmembrane serine protease receptor-2 (TMPRSS2) in COVID-19 (Boson et al., 2021; H. Singh et al., 2021).
Among the various genes possibly linked to COVID-19, the relationship between genetic variations in genes related to the renin-angiotensin-aldosterone system, ACE2 and TMPRSS2, and the severity of the disease have been extensively studied (Glotov et al., 2021). The single nucleotide polymorphisms (SNPs) ACE2 rs2285666 and TMPRSS2 rs12329760 have been investigated in multiple studies, but the results are contradictory (Adimulam et al., 2023; Adli et al., 2022;Fernández-de-las-Peñas et al., 2023; Varillas-Delgado et al., 2023).
Current evidence indicates a significant influence of these polymorphisms on COVID-19, but complicates the understanding of their association with the pathophysiology of the infection (Castanares-Zapatero et al., 2022). Although ACE2 and TMPRSS2 are abundantly expressed in the lungs and respiratory system, explaining the targeting of SARS-CoV-2, they are also present in several other tissues and cells, such as macrophages, heart, muscle and kidney cells and neurons (Zou et al., 2020). This widespread distribution of these receptors explains the possible diversity of symptoms observed during acute infection (Zhirnov & Poyarkov, 2021).
It is important to note that the COVID-19 pandemic has not only resulted in millions of acute cases and deaths, but is also generating a second outbreak, characterized by the persistence of symptoms after the acute phase of the infection, known as long COVID (Fernández-de-las-Peñas, 2022) or post-COVID-19 (Soriano et al., 2022). Recent analysis indicates that around 30-50% of COVID-19 survivors develop persistent symptoms for at least a year after infection (Fernández-de-las-Peñas et al., 2021; Q. Han et al., 2022).
In addition, these polymorphisms influence the expression of ACE2 and TMPRSS2 receptors. For example, the ACE2 rs2285666 polymorphism increases the expression of this gene by up to 50%, which can lead to complications such as vascular constriction, endothelial dysfunction, fibrosis and inflammation (Ni et al., 2020), all suggested as possible causes of post-COVID symptoms (Castanares-Zapatero et al., 2022).
Studies have shown that plasma ACE2 activity remains elevated three months after acute infection in individuals with long COVID, and that the presence of long-term systemic inflammation after the acute phase is associated with more severe symptoms (Patel et al., 2021). Therefore, variants in the ACE2 and TMPRSS2 gene polymorphisms may be linked to the development of post-COVID symptoms (Varillas-Delgado et al., 2023).
Previous studies have investigated the relationship between SNPs and COVID-19 predisposition and severity to identify individual risk factors (Glotov et al., 2021; A. Srivastava et al., 2020). Since the ACE2 and TMPRSS2 polymorphisms were associated with the severity of COVID-19, and considering that severe disease is linked to a higher risk of post-COVID respiratory symptoms (Maglietta et al., 2022), it is plausible that these polymorphisms also influence the development of these symptoms. However, no associations were found between the SNPs investigated (ACE2 rs2285666, ACE2 rs2074192, TMPRSS2 rs12329760, TMPRSS2 rs2070788) and long COVID in previously hospitalized patients, indicating that these polymorphisms do not predispose to these symptoms (Fernández-de-las-Peñas et al., 2023).
The lack of direct genetic influence on long COVID does not rule out a role for the products of the ACE2 and TMPRSS2 genes in these symptoms (Fernández-de-las-Peñas et al., 2023). As previously mentioned, ACE2 plasma activity remains high in individuals with long-standing COVID (Patel et al., 2021), suggesting a possible role for these products, rather than polymorphisms, in the development or maintenance of these symptoms.
It is possible that certain genes influence specific symptoms of long COVID and that ACE genetic polymorphisms are associated with pre-existing comorbidities. Given the high level of ACE2 and TMPRSS2 expression in lung tissue, conditions such as asthma, chronic obstructive pulmonary disease, hypertension and obesity may increase the expression of these receptors (Radzikowska et al., 2020).
The genetic set recognized as the HLA system, located in a highly variable region of human DNA, plays several vital roles in regulating organic defences (Chong et al., 2018). HLA class I antigens play a crucial role in the exposure of foreign material to CD8+ T cells and also interact with existing receptors on NK cells (Bassani-Sternberg & Gfeller, 2016). There is a suspicion that different HLA allelic forms may influence vulnerability to COVID-19, as occurs in other infectious diseases (Campbell et al., 2020). However, comprehensive genetic research has not revealed an HLA predominance in COVID-19 patients in general (Grifoni et al., 2020; Jungreis et al., 2021). The connection between the different HLA varieties and the incidence and severity of COVID-19 varies between population groups and geographical areas (Campbell et al., 2020), possibly due to ethnic diversity and the complexity of the effects generated by HLA-I polymorphisms, which include interaction with different viral fragments, cellular expression and receptors on T and NK cells (Ferretti et al., 2020; Grifoni et al., 2020). Unlike SARS-CoV, SARS-CoV-2 prevents the immune reaction by degrading HLA-I, which may contribute to the lack of a direct relationship between HLA types and COVID-19 outbreaks (Campbell et al., 2020; Kared et al., 2021; Le Bert et al., 2020).
The invasion of SARS-CoV-2 decreases the amount of HLA-I on the cell surface through a gene unique to SARS-CoV-2 that encodes ORF8 (Ferretti et al., 2020). According to the “authorization” scheme, NK cells achieve functional efficiency through a process of instruction facilitated by inhibitory receptors capable of binding to class I auto-HLA molecules (Jungreis et al., 2021). NK cells that have strong inhibitory receptors for their own HLA-I show greater functional reactivity to stimulation, while NK cells without self-specific inhibitory receptors show a reduced response (Campbell et al., 2020). Self-education allows NK cells to identify irregular cells with low surface expression of HLA-I, something common during viral infection (Le Bert et al., 2020). Since suppression of HLA would lead to the inactivity of NK cells and, consequently, to the destruction of target cells, the antiviral response mediated by NK cells may be particularly crucial to exterminate SARS-CoV-2 when T cells lose their ability to recognize target cells (Kared et al., 2021; Le Bert et al., 2020). Discrepancies in the efficacy and strength of NK cells may contribute to individual variations in susceptibility to COVID-19.
Patients with the most severe SARS-CoV-2 outcome had high serum levels of pro-inflammatory cytokines responsible for inducing the cytokine storm (G. Chen et al., 2020; Ruan et al., 2020). Interestingly, most severe cases of COVID-19 with respiratory distress syndrome were associated with elevated systemic levels of IL-1b, TNF and IL-6, suggesting a direct connection between the induction of pro-inflammatory cytokines and the adverse effects of COVID-19 (Huang et al., 2020). Since SARS-CoV-2 has 79% nucleotide identity with SARS-CoV (N. Singh et al., 2020), the main pathogenic mechanisms, including cytokine storm and extensive lung damage during SARS and COVID-19 infection, may be similar. Cytokine storm is a condition caused by the extensive activation of the immune system and, as a result, the extremely high production of cytokines and chemokines. As cytokine storm can lead to multiple organ failure, it is important to understand the mechanisms that drive this condition.
Adaptive immunity is also activated during COVID-19, mainly by antigen-presenting dendritic cells, which produce large amounts of cytokines, including IL-6, IL-1b and TNF, and migrate to regional lymph nodes to present the viral antigen to virgin T cells, pushing their differentiation and migration to the affected tissue (Monteleone et al., 2020). The specific humoral response represented by B cells producing virus-specific antibodies is also present (Guo et al., 2020). The replication of the virus results in additional damage to the affected organs, along with a self-reinforcing immune response, manifesting itself in the uncontrolled overexpression of inflammatory mediators in severe cases. Another mechanism that drives the cytokine storm during viral infections is the increased permeability of blood vessels, which allows the infiltration of effector cells, producing additional quantities of inflammatory molecules and exacerbating the production of hypercytokines (Tisoncik et al., 2012). In addition, leaky blood vessels allow the virus to spread to other tissues and organs, compromising their functions. Finally, under the persistence of inflammatory factors, an increased number of inflammatory exudates and erythrocytes enter the alveoli, resulting in lung damage and respiratory failure.
IL-6 is a cytokine with multiple functions, from blood cell formation and metabolic regulation to inflammation, autoimmunity and acute immune response. IL-6 influences the body’s defense through various immunological mechanisms: it controls the activity of monocytes and their transformation into macrophages (Chomarat et al., 2000), regulates the differentiation of B cells in response to antigens (Urashima et al., 1996), increases IgG production by B cells (R. Yang et al., 2016) and favors the Th2 immune response by inhibiting Th1 polarization (Diehl & Rincón, 2002). Several studies have shown a strong link between IL-6 levels in the blood and the subsequent development of respiratory failure (X. Chen et al., 2020; Coomes & Haghbayan, 2020). Even moderately high levels of IL-6 above 80 pg/mL were enough to identify COVID-19 patients at high risk of respiratory failure (Herold et al., 2020). In addition, the SARS-CoV-2 viral RNA present in the blood, which is strongly related to the cytokine storm, is closely linked to the extremely high levels of IL-6 in the blood (X. Chen et al., 2020). It is also suggested that continuous measurement of circulating IL-6 may be crucial to monitor disease progression or, when assessed soon after COVID-19 diagnosis, may predict the next occurrence of respiratory failure or, alternatively, the presence of asymptomatic infection in SARS-CoV-2 infected patients. (Ulhaq & Soraya, 2020).
CONCLUSION
Given the complexity and severity of the COVID-19 pandemic, it is clear that its repercussions go beyond the acute phase of the infection. The post-COVID syndrome, known as long COVID, is emerging as a multi-systemic condition that considerably impacts patients’ quality of life, manifesting itself in a wide variety of physical and mental symptoms. In this context, understanding the mechanisms underlying this syndrome, including virological and genetic factors, is fundamental to guiding the development of effective diagnosis, treatment and recovery strategies. However, much remains to be unraveled about COVID-19 and its long-term implications, underscoring the continued importance of research and epidemiological surveillance to address this global health challenge. Thus, given the complexity of both COVID-19 and the post-COVID syndrome, it is crucial to persist in research to elucidate the mechanisms behind long COVID. The studies reviewed highlight the relevance of genetic markers such as ACE2, TMPRSS2, HLA-1, IL-6 in the predisposition and severity of the disease, pointing to a possible association between these polymorphisms and persistent symptoms. However, further research is imperative to fully understand the role of these genes and other factors in post-COVID syndrome, with a view to developing effective treatment and management approaches for affected patients.
REFERENCES
Adimulam, T., Arumugam, T., Naidoo, A., Naidoo, K., & Ramsuran, V. (2023). Polymorphisms within the SARS-CoV-2 Human Receptor Genes Associate with Variable Disease Outcomes across Ethnicities. Genes, 14(9), 1798. https://doi.org/10.3390/genes14091798
Adli, A., Rahimi, M., Khodaie, R., Hashemzaei, N., & Hosseini, S. M. (2022). Role of genetic variants and host polymorphisms on COVID‐19: From viral entrance mechanisms to immunological reactions. Journal of Medical Virology, 94(5), 1846–1865. https://doi.org/10.1002/jmv.27615
Al-Aly, Z., Xie, Y., & Bowe, B. (2021). High-dimensional characterization of post-acute sequelae of COVID-19. Nature, 594(7862), 259–264. https://doi.org/10.1038/s41586-021-03553-9
Bárbara Chiocca Do Nascimento, C., Marchiori, M. F., Campo, V. L., Magalhães, M., & Zini, C. (2020). SARS-CoV2 e Covid-19: aspectos fisiopatológicos e imunológicos, estratégias de diagnóstico e desenvolvimento de vacinas SARS-CoV2 and Covid-19: pathophysiological and immunological aspects, diagnostic strategies and vaccine development. 2.
Bassani-Sternberg, M., & Gfeller, D. (2016). Unsupervised HLA Peptidome Deconvolution Improves Ligand Prediction Accuracy and Predicts Cooperative Effects in Peptide–HLA Interactions. The Journal of Immunology, 197(6), 2492–2499. https://doi.org/10.4049/jimmunol.1600808
Boson, B., Legros, V., Zhou, B., Siret, E., Mathieu, C., Cosset, F.-L., Lavillette, D., & Denolly, S. (2021). The SARS-CoV-2 envelope and membrane proteins modulate maturation and retention of the spike protein, allowing assembly of virus-like particles. Journal of Biological Chemistry, 296, 100111. https://doi.org/10.1074/jbc.RA120.016175
BRASIL. Ministério da Saúde. (2021). https://covid.saude.gov.br/. https://covid.saude.gov.br/
BRASIL. Ministério da Saúde. (2024). https://covid.saude.gov.br/. https://covid.saude.gov.br/
Campbell, K. M., Steiner, G., Wells, D. K., Ribas, A., & Kalbasi, A. (2020). Prioritization of SARS-CoV-2 epitopes using a pan-HLA and global population inference approach. BioRxiv : The Preprint Server for Biology. https://doi.org/10.1101/2020.03.30.016931
Cao, Y., Yang, R., Lee, I., Zhang, W., Sun, J., Wang, W., & Meng, X. (2021). Characterization of the <scp>SARS‐CoV</scp> ‐2 E Protein: Sequence, Structure, Viroporin, and Inhibitors. Protein Science, 30(6), 1114–1130. https://doi.org/10.1002/pro.4075
Castanares-Zapatero, D., Chalon, P., Kohn, L., Dauvrin, M., Detollenaere, J., Maertens de Noordhout, C., Primus-de Jong, C., Cleemput, I., & Van den Heede, K. (2022). Pathophysiology and mechanism of long COVID: a comprehensive review. Annals of Medicine, 54(1), 1473–1487. https://doi.org/10.1080/07853890.2022.2076901
Chen, G., Wu, D., Guo, W., Cao, Y., Huang, D., Wang, H., Wang, T., Zhang, X., Chen, H., Yu, H., Zhang, X., Zhang, M., Wu, S., Song, J., Chen, T., Han, M., Li, S., Luo, X., Zhao, J., & Ning, Q. (2020). Clinical and immunological features of severe and moderate coronavirus disease 2019. Journal of Clinical Investigation, 130(5), 2620–2629. https://doi.org/10.1172/JCI137244
Chen, X., Zhao, B., Qu, Y., Chen, Y., Xiong, J., Feng, Y., Men, D., Huang, Q., Liu, Y., Yang, B., Ding, J., & Li, F. (2020). Detectable Serum Severe Acute Respiratory Syndrome Coronavirus 2 Viral Load (RNAemia) Is Closely Correlated With Drastically Elevated Interleukin 6 Level in Critically Ill Patients With Coronavirus Disease 2019. Clinical Infectious Diseases, 71(8), 1937–1942. https://doi.org/10.1093/cid/ciaa449
Chen, Z., Zhang, P., Matsuoka, Y., Tsybovsky, Y., West, K., Santos, C., Boyd, L. F., Nguyen, H., Pomerenke, A., Stephens, T., Olia, A. S., Zhang, B., De Giorgi, V., Holbrook, M. R., Gross, R., Postnikova, E., Garza, N. L., Johnson, R. F., Margulies, D. H., … Farci, P. (2022). Potent monoclonal antibodies neutralize Omicron sublineages and other SARS-CoV-2 variants. Cell Reports, 41(5), 111528. https://doi.org/10.1016/j.celrep.2022.111528
Chomarat, P., Banchereau, J., Davoust, J., & Karolina Palucka, A. (2000). IL-6 switches the differentiation of monocytes from dendritic cells to macrophages. Nature Immunology, 1(6), 510–514. https://doi.org/10.1038/82763
Chong, C., Marino, F., Pak, H., Racle, J., Daniel, R. T., Müller, M., Gfeller, D., Coukos, G., & Bassani-Sternberg, M. (2018). High-throughput and Sensitive Immunopeptidomics Platform Reveals Profound Interferonγ-Mediated Remodeling of the Human Leukocyte Antigen (HLA) Ligandome. Molecular & Cellular Proteomics, 17(3), 533–548. https://doi.org/10.1074/mcp.TIR117.000383
Coomes, E. A., & Haghbayan, H. (2020). Interleukin‐6 in Covid‐19: A systematic review and <scp>meta‐analysis</scp>. Reviews in Medical Virology, 30(6), 1–9. https://doi.org/10.1002/rmv.2141
Costa Da Costa, T. D., Da, F., Ribeiro, S., De, G., & Pires Da Silva, J. (2023). CAPACIDADE FUNCIONAL DE PACIENTES PÓS COVID-19 E FATORES ASSOCIADOS 1 FUNCTIONAL CAPACITY OF POST COVID-19 PATIENTS AND ASSOCIATED FACTORS CAPACIDAD FUNCIONAL DE LOS PACIENTES TRAS EL COVID-19 Y FACTORES ASOCIADOS. Revista de Estudos Multidisciplinares, 1.
Da Silva, C. C., De Carvalho, C. M. O., De Lima, D. C., Costa, E. S., De Andrade, V. M. B., Tenorio, B. M., Britto, D. B. L. de A., & Tenorio, F. C. A. M. (2021). Covid-19: Aspectos da origem, fisiopatologia, imunologia e tratamento – uma revisão narrativa. Revista Eletrônica Acervo Saúde, 13(3), e6542. https://doi.org/10.25248/reas.e6542.2021
Diehl, S., & Rincón, M. (2002). The two faces of IL-6 on Th1/Th2 differentiation. Molecular Immunology, 39(9), 531–536. https://doi.org/10.1016/S0161-5890(02)00210-9
Fernández-de-las-Peñas, C. (2022). Long COVID: current definition. Infection, 50(1), 285–286. https://doi.org/10.1007/s15010-021-01696-5
Fernández-de-las-Peñas, C., Arendt-Nielsen, L., Díaz-Gil, G., Gómez-Esquer, F., Gil-Crujera, A., Gómez-Sánchez, S. M., Ambite-Quesada, S., Palomar-Gallego, M. A., Pellicer-Valero, O. J., & Giordano, R. (2022). Genetic Association between ACE2 (rs2285666 and rs2074192) and TMPRSS2 (rs12329760 and rs2070788) Polymorphisms with Post-COVID Symptoms in Previously Hospitalized COVID-19 Survivors. Genes, 13(11), 1935. https://doi.org/10.3390/genes13111935
Fernández-de-las-Peñas, C., Arendt-Nielsen, L., Díaz-Gil, G., Gómez-Esquer, F., Gil-Crujera, A., Gómez-Sánchez, S. M., Ambite-Quesada, S., Palomar-Gallego, M. A., Pellicer-Valero, O. J., & Giordano, R. (2023). Apolipoprotein E (ApoE) ε4 Genotype (ApoE rs429358—ApoE rs7412 Polymorphisms) Is Not Associated with Long COVID Symptoms in Previously Hospitalized COVID-19 Survivors. Genes, 14(7), 1420. https://doi.org/10.3390/genes14071420
Fernández-de-las-Peñas, C., Palacios-Ceña, D., Gómez-Mayordomo, V., Florencio, L. L., Cuadrado, M. L., Plaza-Manzano, G., & Navarro-Santana, M. (2021). Prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: A systematic review and meta-analysis. European Journal of Internal Medicine, 92, 55–70. https://doi.org/10.1016/j.ejim.2021.06.009
Ferretti, A. P., Kula, T., Wang, Y., Nguyen, D. M. V., Weinheimer, A., Dunlap, G. S., Xu, Q., Nabilsi, N., Perullo, C. R., Cristofaro, A. W., Whitton, H. J., Virbasius, A., Olivier, K. J., Buckner, L. R., Alistar, A. T., Whitman, E. D., Bertino, S. A., Chattopadhyay, S., & MacBeath, G. (2020). Unbiased Screens Show CD8+ T Cells of COVID-19 Patients Recognize Shared Epitopes in SARS-CoV-2 that Largely Reside outside the Spike Protein. Immunity, 53(5), 1095-1107.e3. https://doi.org/10.1016/j.immuni.2020.10.006
Glotov, O. S., Chernov, A. N., Scherbak, S. G., & Baranov, V. S. (2021). Genetic Risk Factors for the Development of COVID-19 Coronavirus Infection. Russian Journal of Genetics, 57(8), 878–892. https://doi.org/10.1134/S1022795421080056
Gorbalenya, A. E., Baker, S. C., Baric, R. S., de Groot, R. J., Drosten, C., Gulyaeva, A. A., Haagmans, B. L., Lauber, C., Leontovich, A. M., Neuman, B. W., Penzar, D., Perlman, S., Poon, L. L. M., Samborskiy, D. V., Sidorov, I. A., Sola, I., & Ziebuhr, J. (2020). The species Severe acute respiratory syndrome-related coronavirus: classifying 2019-nCoV and naming it SARS-CoV-2. Nature Microbiology, 5(4), 536–544. https://doi.org/10.1038/s41564-020-0695-z
Grifoni, A., Weiskopf, D., Ramirez, S. I., Mateus, J., Dan, J. M., Moderbacher, C. R., Rawlings, S. A., Sutherland, A., Premkumar, L., Jadi, R. S., Marrama, D., de Silva, A. M., Frazier, A., Carlin, A. F., Greenbaum, J. A., Peters, B., Krammer, F., Smith, D. M., Crotty, S., & Sette, A. (2020). Targets of T Cell Responses to SARS-CoV-2 Coronavirus in Humans with COVID-19 Disease and Unexposed Individuals. Cell, 181(7), 1489-1501.e15. https://doi.org/10.1016/j.cell.2020.05.015
Guo, C., Li, B., Ma, H., Wang, X., Cai, P., Yu, Q., Zhu, L., Jin, L., Jiang, C., Fang, J., Liu, Q., Zong, D., Zhang, W., Lu, Y., Li, K., Gao, X., Fu, B., Liu, L., Ma, X., … Qu, K. (2020). Single-cell analysis of two severe COVID-19 patients reveals a monocyte-associated and tocilizumab-responding cytokine storm. Nature Communications, 11(1), 3924. https://doi.org/10.1038/s41467-020-17834-w
Han, M. S., Choi, E. H., Chang, S. H., Jin, B.-L., Lee, E. J., Kim, B. N., Kim, M. K., Doo, K., Seo, J.-H., Kim, Y.-J., Kim, Y. J., Park, J. Y., Suh, S. B., Lee, H., Cho, E. Y., Kim, D. H., Kim, J. M., Kim, H. Y., Park, S. E., … Kim, J.-H. (2021). Clinical Characteristics and Viral RNA Detection in Children With Coronavirus Disease 2019 in the Republic of Korea. JAMA Pediatrics, 175(1), 73. https://doi.org/10.1001/jamapediatrics.2020.3988
Han, Q., Zheng, B., Daines, L., & Sheikh, A. (2022). Long-Term Sequelae of COVID-19: A Systematic Review and Meta-Analysis of One-Year Follow-Up Studies on Post-COVID Symptoms. Pathogens, 11(2), 269. https://doi.org/10.3390/pathogens11020269
Herold, T., Jurinovic Phd, V., Arnreich, C., Hellmuth, J. C., Von Bergwelt-Baildon, M., Klein, M., & Weinberger, T. (2020). Level of IL-6 predicts respiratory failure in hospitalized symptomatic COVID-19 patients. https://doi.org/10.1101/2020.04.01.20047381
Hou, Y., Zhao, J., Martin, W., Kallianpur, A., Chung, M. K., Jehi, L., Sharifi, N., Erzurum, S., Eng, C., & Cheng, F. (2020). New insights into genetic susceptibility of COVID-19: an ACE2 and TMPRSS2 polymorphism analysis. BMC Medicine, 18(1), 216. https://doi.org/10.1186/s12916-020-01673-z
Huang, C., Wang, Y., Li, X., Ren, L., Zhao, J., Hu, Y., Zhang, L., Fan, G., Xu, J., Gu, X., Cheng, Z., Yu, T., Xia, J., Wei, Y., Wu, W., Xie, X., Yin, W., Li, H., Liu, M., … Cao, B. (2020). Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet, 395(10223), 497–506. https://doi.org/10.1016/S0140-6736(20)30183-5
Iqbal, A., Iqbal, K., Arshad Ali, S., Azim, D., Farid, E., Baig, M. D., Bin Arif, T., & Raza, M. (2021). The COVID-19 Sequelae: A Cross-Sectional Evaluation of Post-recovery Symptoms and the Need for Rehabilitation of COVID-19 Survivors. Cureus. https://doi.org/10.7759/cureus.13080
Jungreis, I., Nelson, C. W., Ardern, Z., Finkel, Y., Krogan, N. J., Sato, K., Ziebuhr, J., Stern-Ginossar, N., Pavesi, A., Firth, A. E., Gorbalenya, A. E., & Kellis, M. (2021). Conflicting and ambiguous names of overlapping ORFs in the SARS-CoV-2 genome: A homology-based resolution. Virology, 558, 145–151. https://doi.org/10.1016/j.virol.2021.02.013
Kared, H., Redd, A. D., Bloch, E. M., Bonny, T. S., Sumatoh, H., Kairi, F., Carbajo, D., Abel, B., Newell, E. W., Bettinotti, M. P., Benner, S. E., Patel, E. U., Littlefield, K., Laeyendecker, O., Shoham, S., Sullivan, D., Casadevall, A., Pekosz, A., Nardin, A., … Quinn, T. C. (2021). SARS-CoV-2–specific CD8+ T cell responses in convalescent COVID-19 individuals. Journal of Clinical Investigation, 131(5). https://doi.org/10.1172/JCI145476
Le Bert, N., Tan, A. T., Kunasegaran, K., Tham, C. Y. L., Hafezi, M., Chia, A., Chng, M. H. Y., Lin, M., Tan, N., Linster, M., Chia, W. N., Chen, M. I.-C., Wang, L.-F., Ooi, E. E., Kalimuddin, S., Tambyah, P. A., Low, J. G.-H., Tan, Y.-J., & Bertoletti, A. (2020). SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls. Nature, 584(7821), 457–462. https://doi.org/10.1038/s41586-020-2550-z
Maglietta, G., Diodati, F., Puntoni, M., Lazzarelli, S., Marcomini, B., Patrizi, L., & Caminiti, C. (2022). Prognostic Factors for Post-COVID-19 Syndrome: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(6), 1541. https://doi.org/10.3390/jcm11061541
Meng, Z., Guo, S., Zhou, Y., Li, M., Wang, M., & Ying, B. (2021). Applications of laboratory findings in the prevention, diagnosis, treatment, and monitoring of COVID-19. Signal Transduction and Targeted Therapy, 6(1), 316. https://doi.org/10.1038/s41392-021-00731-z
Monteleone, G., Sarzi-Puttini, P. C., & Ardizzone, S. (2020). Preventing COVID-19-induced pneumonia with anticytokine therapy. The Lancet Rheumatology, 2(5), e255–e256. https://doi.org/10.1016/S2665-9913(20)30092-8
Ni, W., Yang, X., Yang, D., Bao, J., Li, R., Xiao, Y., Hou, C., Wang, H., Liu, J., Yang, D., Xu, Y., Cao, Z., & Gao, Z. (2020). Role of angiotensin-converting enzyme 2 (ACE2) in COVID-19. Critical Care, 24(1), 422. https://doi.org/10.1186/s13054-020-03120-0
Nunes, M. de C., Alves, O. N., Santana, L. C. de, & Nunes, L. T. D. (2022). Síndrome da COVID longa: uma revisão integrativa. Research, Society and Development, 11(13), e572111335990. https://doi.org/10.33448/rsd-v11i13.35990
Patel, S. K., Juno, J. A., Lee, W. S., Wragg, K. M., Hogarth, P. M., Kent, S. J., & Burrell, L. M. (2021). Plasma ACE2 activity is persistently elevated following SARS-CoV-2 infection: implications for COVID-19 pathogenesis and consequences. European Respiratory Journal, 57(5), 2003730. https://doi.org/10.1183/13993003.03730-2020
Radzikowska, U., Ding, M., Tan, G., Zhakparov, D., Peng, Y., Wawrzyniak, P., Wang, M., Li, S., Morita, H., Altunbulakli, C., Reiger, M., Neumann, A. U., Lunjani, N., Traidl‐Hoffmann, C., Nadeau, K. C., O’Mahony, L., Akdis, C., & Sokolowska, M. (2020). Distribution of ACE2, CD147, CD26, and other SARS‐CoV‐2 associated molecules in tissues and immune cells in health and in asthma, COPD, obesity, hypertension, and COVID‐19 risk factors. Allergy, 75(11), 2829–2845. https://doi.org/10.1111/all.14429
Ramos, F., Carvalho1, S., Gobbi2, L. C., Casotti2, G. C., Dias Lyra2, M. E., Tiussi2, L. M., Julia, A., Caetano2, F., Luiza, A., Cavalari2, C., Lopes Pinheiro2, M. I., & Carrijo-Carvalho3, L. C. (2020). FISIOPATOLOGIA DA COVID-19: REPERCUSSÕES SISTÊMICAS COVID-19 PATHOPHYSIOLOGY: SYSTEMIC REPERCUSSIONS.
Reser, M. R. (2021). Polimorfismo da ACE2 e a Influência na Suscetibilidade frente à COVID-19 / ACE2 Polymorphism and the Influence on Susceptibility to COVID-19. Brazilian Journal of Development, 7(9), 91868–91879. https://doi.org/10.34117/bjdv7n9-379
Rojas, M., Rodríguez, Y., Acosta-Ampudia, Y., Monsalve, D. M., Zhu, C., Li, Q.-Z., Ramírez-Santana, C., & Anaya, J.-M. (2022). Autoimmunity is a hallmark of post-COVID syndrome. Journal of Translational Medicine, 20(1), 129. https://doi.org/10.1186/s12967-022-03328-4
Ruan, Q., Yang, K., Wang, W., Jiang, L., & Song, J. (2020). Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Medicine, 46(5), 846–848. https://doi.org/10.1007/s00134-020-05991-x
Saadi, F., Pal, D., & Sarma, J. Das. (2021). Spike Glycoprotein Is Central to Coronavirus Pathogenesis-Parallel Between m-CoV and SARS-CoV-2. Annals of Neurosciences, 28(3–4), 201–218. https://doi.org/10.1177/09727531211023755
SANTOS FILHO, A. dos, & LIMA, Alessandra. (2021). covid-19-covid-longa-e-pos-covid.
Shah, S., Danda, D., Kavadichanda, C., Das, S., Adarsh, M. B., & Negi, V. S. (2020). Autoimmune and rheumatic musculoskeletal diseases as a consequence of SARS-CoV-2 infection and its treatment. Rheumatology International, 40(10), 1539–1554. https://doi.org/10.1007/s00296-020-04639-9
Shalev, A., Liberzon, I., & Marmar, C. (2017). Post-Traumatic Stress Disorder. New England Journal of Medicine, 376(25), 2459–2469. https://doi.org/10.1056/NEJMra1612499
Singh, H., Choudhari, R., Nema, V., & Khan, A. A. (2021). ACE2 and TMPRSS2 polymorphisms in various diseases with special reference to its impact on COVID-19 disease. Microbial Pathogenesis, 150, 104621. https://doi.org/10.1016/j.micpath.2020.104621
Singh, N., Rai, S. N., Singh, V., & Singh, M. P. (2020). Molecular characterization, pathogen-host interaction pathway and in silico approaches for vaccine design against COVID-19. Journal of Chemical Neuroanatomy, 110, 101874. https://doi.org/10.1016/j.jchemneu.2020.101874
Soriano, J. B., Murthy, S., Marshall, J. C., Relan, P., & Diaz, J. V. (2022). A clinical case definition of post-COVID-19 condition by a Delphi consensus. The Lancet Infectious Diseases, 22(4), e102–e107. https://doi.org/10.1016/S1473-3099(21)00703-9
Srivastava, A., Bandopadhyay, A., Das, D., Pandey, R. K., Singh, V., Khanam, N., Srivastava, N., Singh, P. P., Dubey, P. K., Pathak, A., Gupta, P., Rai, N., Sultana, G. N. N., & Chaubey, G. (2020). Genetic Association of ACE2 rs2285666 Polymorphism With COVID-19 Spatial Distribution in India. Frontiers in Genetics, 11. https://doi.org/10.3389/fgene.2020.564741
Srivastava, M., Hall, D., Omoru, O. B., Gill, H. M., Smith, S., & Janga, S. C. (2021). Mutational Landscape and Interaction of SARS-CoV-2 with Host Cellular Components. Microorganisms, 9(9), 1794. https://doi.org/10.3390/microorganisms9091794
Sun, L., Li, P., Ju, X., Rao, J., Huang, W., Ren, L., Zhang, S., Xiong, T., Xu, K., Zhou, X., Gong, M., Miska, E., Ding, Q., Wang, J., & Zhang, Q. C. (2021). In vivo structural characterization of the SARS-CoV-2 RNA genome identifies host proteins vulnerable to repurposed drugs. Cell, 184(7), 1865-1883.e20. https://doi.org/10.1016/j.cell.2021.02.008
Tisoncik, J. R., Korth, M. J., Simmons, C. P., Farrar, J., Martin, T. R., & Katze, M. G. (2012). Into the Eye of the Cytokine Storm. Microbiology and Molecular Biology Reviews, 76(1), 16–32. https://doi.org/10.1128/MMBR.05015-11
Townsend, L., Dyer, A. H., Jones, K., Dunne, J., Mooney, A., Gaffney, F., O’Connor, L., Leavy, D., O’Brien, K., Dowds, J., Sugrue, J. A., Hopkins, D., Martin-Loeches, I., Ni Cheallaigh, C., Nadarajan, P., McLaughlin, A. M., Bourke, N. M., Bergin, C., O’Farrelly, C., … Conlon, N. (2020). Persistent fatigue following SARS-CoV-2 infection is common and independent of severity of initial infection. PLOS ONE, 15(11), e0240784. https://doi.org/10.1371/journal.pone.0240784
Ulhaq, Z. S., & Soraya, G. V. (2020). Interleukin-6 as a potential biomarker of COVID-19 progression. Médecine et Maladies Infectieuses, 50(4), 382–383. https://doi.org/10.1016/j.medmal.2020.04.002
Urashima, M., Chauhan, D., Hatziyanni, M., Ogata, A., Hollenbaugh, D., Aruffo, A., & Anderson, K. C. (1996). CD40 ligand triggers interleukin-6 mediated B cell differentiation. Leukemia Research, 20(6), 507–515. https://doi.org/10.1016/0145-2126(95)00098-4
Varillas-Delgado, D., Jimenez-Antona, C., Lizcano-Alvarez, A., Cano-de-la-Cuerda, R., Molero-Sanchez, A., & Laguarta-Val, S. (2023). Predictive Factors and ACE-2 Gene Polymorphisms in Susceptibility to Long COVID-19 Syndrome. International Journal of Molecular Sciences, 24(23), 16717. https://doi.org/10.3390/ijms242316717
Xie, Y., & Al-Aly, Z. (2022). Risks and burdens of incident diabetes in long COVID: a cohort study. The Lancet Diabetes & Endocrinology, 10(5), 311–321. https://doi.org/10.1016/S2213-8587(22)00044-4
Yang, R., Masters, A. R., Fortner, K. A., Champagne, D. P., Yanguas-Casás, N., Silberger, D. J., Weaver, C. T., Haynes, L., & Rincon, M. (2016). IL-6 promotes the differentiation of a subset of naive CD8+ T cells into IL-21–producing B helper CD8+ T cells. Journal of Experimental Medicine, 213(11), 2281–2291. https://doi.org/10.1084/jem.20160417
Yang, T., Yan, M. Z., Li, X., & Lau, E. H. Y. (2022). Sequelae of COVID-19 among previously hospitalized patients up to 1 year after discharge: a systematic review and meta-analysis. Infection, 50(5), 1067–1109. https://doi.org/10.1007/s15010-022-01862-3
Zhirnov, O. P., & Poyarkov, S. V. (2021). Novel Negative Sense Genes in the RNA Genome of Coronaviruses. Doklady Biochemistry and Biophysics, 496(1), 27–31. https://doi.org/10.1134/S1607672921010130
Zou, X., Chen, K., Zou, J., Han, P., Hao, J., & Han, Z. (2020). Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Frontiers of Medicine, 14(2), 185–192. https://doi.org/10.1007/s11684-020-0754-0
1 Faculdade Metropolitana-UNNESA, Rua das Ararás, 241 – Eldorado, Porto Velho – RO, 76811-678, Brasil,
2 Laboratório de Virologia Molecular- Fundação Oswaldo Cruz Rondônia FIOCRUZ/RO, Rua da Beira, 7176, Porto Velho 76812‑245, Brazil;
3 Centro de Pesquisa em Medicina Tropical – CEPEM, Porto Velho, RO, Brazil
4 Programa de Pós‑Graduação em Biologia Experimental, Universidade Federal de Rondônia | Fiocruz-RO.
5 Instituto Nacional de Ciência e Tecnologia de Epidemiologia da Amazônia Ocidental – INCT-EpiAmO, 76812-245, Porto Velho, RO, Brazil