REGISTRO DOI: 10.69849/revistaft/ra10202511140914
Felipe Muniz da Cunha¹
André William Masseaux Vidal Júnior²
Marcelle Andrade da Conceição³
Abstract
Canine cranial cruciate ligament disease (CCLD) is one of the main orthopedic conditions in dogs, characterized by degenerative or traumatic changes of the cranial cruciate ligament (CCL). It primarily affects large and giant breeds but can also occur in small breeds, especially when medial patellar luxation (MPL) is associated. The objective was to report the feasibility and efficacy of the simultaneous mTPLO technique in the concomitant treatment of medial patellar luxation and cranial cruciate ligament disease in a dog, which was subsequently submitted to a modified TPLO surgical technique for simultaneous correction of both orthopedic conditions. Patellar alignment, functional recovery, surgical time, and immediate postoperative discomfort were evaluated. The technique promoted effective restoration of patellar alignment and improvement of locomotor function, with no significant complications observed. Additionally, a reduction in the number of required osteotomies was noted, contributing to shorter surgical time and greater postoperative comfort. The modified TPLO proved to be a promising surgical alternative for the simultaneous treatment of MPL and CCLD, favoring prognosis and patient quality of life. However, studies with a larger number of cases and long-term follow-up are necessary to validate these findings.
Keywords: Modified tibial plateau leveling osteotomy; medial patellar luxation; cranial cruciate ligament disease; veterinary orthopedics; small animal surgery.
Resumo
A doença do ligamento cruzado cranial canino (CCLD) é uma das principais afecções ortopédicas em cães, caracterizadas por alterações degenerativas ou traumáticas do ligamento cruzado cranial (LCCr). Afeta principalmente cães de raças grandes e gigantes, mas também pode ocorrer em raças pequenas, especialmente quando há luxação patelar medial (MLP) associada. O objetivo foi relatar a viabilidade e a eficácia da técnica simultânea de mTPLO no tratamento concomitante da luxação patelar medial e da doença do ligamento cruzado cranial em um cão, posteriormente foi submetido a técnica cirúrgica de TPLO modificada para correção simultânea das duas afecções ortopédicas. Foram avaliados o alinhamento patelar, a recuperação funcional, o tempo cirúrgico e o desconforto no pós-operatório imediato. A técnica promoveu restauração efetiva do alinhamento patelar e melhora da função locomotora, com ausência de complicações relevantes, o paciente foi acompanhado 30 dias, 60 dias e 180 dias depois da cirurgia. Observou-se ainda, a redução de osteotomias necessárias, o que contribuiu para menor tempo cirúrgico e maior conforto no pós-operatório. A TPLO modificada mostrou-se uma alternativa cirúrgica promissora para o tratamento simultâneo de MPL e CCLD, favorecendo o prognóstico e a qualidade de vida do paciente. No entanto, são necessários estudos com maior numero de casos e acompanhamento em longo prazo para validar esses achados.
Palavras chaves: osteotomia niveladora do platô tibial modificada; luxação patelar medial; doença do ligamento cruzado cranial; ortopedia veterinária; cirurgia de pequenos animais.
Introduction
Canine cranial cruciate ligament disease (CCLD) encompasses degenerative or traumatic alterations of the cranial cruciate ligament (CrCL), including partial or complete rupture, laxity, and inflammation. It represents one of the most common orthopedic disorders in dogs, with a higher prevalence in large and giant breeds. However, small breeds such as Shih Tzu, Yorkshire Terrier, and Poodle may also be affected, particularly when medial patellar luxation (MPL) is present, a condition that secondarily compromises ligament stability (Comeford et al., 2011; Conzemius et al., 2005; Moretti et al., 2021). The association between CCLD and MPL induces multi-axial instability, accelerating cartilage wear, pain, and progression to osteoarthritis.
The cranial cruciate ligament plays a crucial role in stabilizing the stifle joint during locomotion, limiting cranial tibial displacement relative to the femur, internal tibial rotation, and joint hyperextension (Arnoczky & Marshall, 1977; Tashman et al., 2004). Loss of its integrity predisposes to meniscal injury, progressive cartilage degeneration, and biomechanical alterations consistent with cranial tibial drawer motion (Brandt et al., 1991).
CrCL injuries may be classified as degenerative or traumatic. The degenerative form, most frequently observed in small to medium-sized middle-aged to elderly dogs, is characterized by progressive ligament weakening and partial or complete rupture. The traumatic form, on the other hand, typically occurs in young large-breed dogs and is commonly associated with intense physical exertion, running, or jumping (Rafla et al., 2025).
Diagnosis is based on clinical history, progression of lameness, physical examination, and specific orthopedic tests. The cranial drawer and tibial compression tests are considered the gold standard for confirming instability (Fossum, 2019; Rafla et al., 2025; Marino & Loughin, 2010). Complementary imaging exams are useful for evaluating osteoarthritic changes and surgical planning.
Surgical management is regarded as the treatment of choice, enabling restoration of joint stability and functional improvement (B. Slocum & T. Slocum, 1993). In small-breed dogs, conservative treatment may be adopted in selected cases, although surgical intervention is indicated in severe conditions (Rafla et al., 2025). Among available surgical techniques, extracapsular, intracapsular, and osteotomy-based procedures are most prominent. The tibial plateau leveling osteotomy (TPLO) is widely performed, as it provides dynamic stability during the stance phase by reducing the tibial plateau angle (Slocum, 1993).
In cases involving concurrent CCLD and MPL, simultaneous correction poses a considerable challenge. Tibial tuberosity transposition (TTT) may be combined with TPLO; however, it carries a risk of tibial osteotomy instability. Consequently, modified techniques such as the modified TPLO (mTPLO) have been developed to correct both conditions. The mTPLO incorporates rotation of the distal tibial fragment to correct alignment deviations, combined with tibial tuberosity transposition, and stabilization with a TPLO plate and Kirschner wires (Livet et al., 2019).
Given this scenario, the objective of this report was to describe the application of mTPLO in a female Yorkshire Terrier, highlighting its effectiveness in the simultaneous correction of CCLD and MPL, as well as its clinical and surgical outcomes.
Case Report
A seven-year-old female Yorkshire Terrier was presented with a one-week history of left pelvic limb lameness and non-weight bearing. The animal had been previously treated with metamizole (25 mg/kg) without satisfactory response.
On orthopedic examination, cranial drawer and tibial compression tests were positive. Patellar instability testing revealed a grade II patellar luxation. Radiographic evaluation demonstrated narrowing of the femorotibial joint space, incongruence of the femoropatellar joint, caudal displacement of the left patella on the mediolateral view, and medial displacement on the craniocaudal view. Additionally, a pronounced cranial deviation of the tibial plateau relative to the femoral condyles was observed. Based on these clinical and radiographic findings, a diagnosis of patellar luxation associated with joint effusion and cranial cruciate ligament insufficiency was established (Figures 1 and 2).
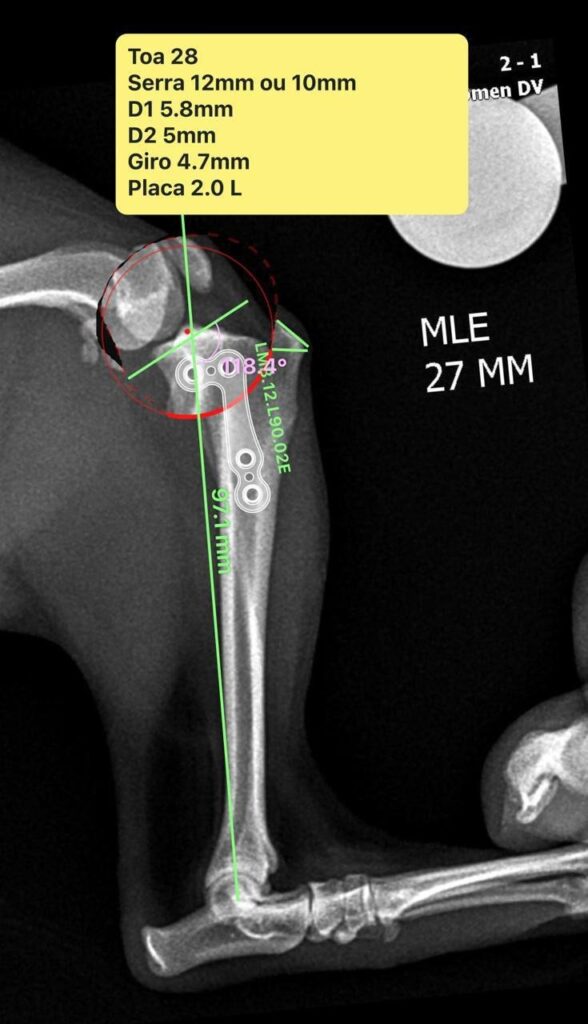
Surgical treatment was selected, consisting of a modified TPLO combined with trochleoplasty to address both conditions. Surgical planning, using a radial TPLO cut, was performed with Vpop Pro® software following the described method for measuring the patellar ligament angle (PLA) relative to the tibial plateau, which was 118.4° (Figure 3).
A medial tibial incision was performed, followed by blunt dissection of the adjacent musculature to expose the bone and identify the medial collateral ligament. The tibial osteotomy was performed with a TPLO-specific saw. The osteotomized tibial segment was rotated using a pointed reduction forceps and temporarily stabilized with a Steinmann pin until plate fixation. Definitive fixation was achieved with a TPLO plate and screws. A Mitzan® orthopedic drill with a 2.0 mm bit was used, guided by the plate’s drilling template. The proximal hole was drilled first, followed by the distal and remaining holes. The Steinmann pin was removed after final fixation, ensuring osteotomy stability.
In this modified technique, the plate was positioned with slight pre-torsion, and the proximal tibial fragment was placed more medially compared to the conventional TPLO configuration. Total surgical time was approximately 50 minutes.
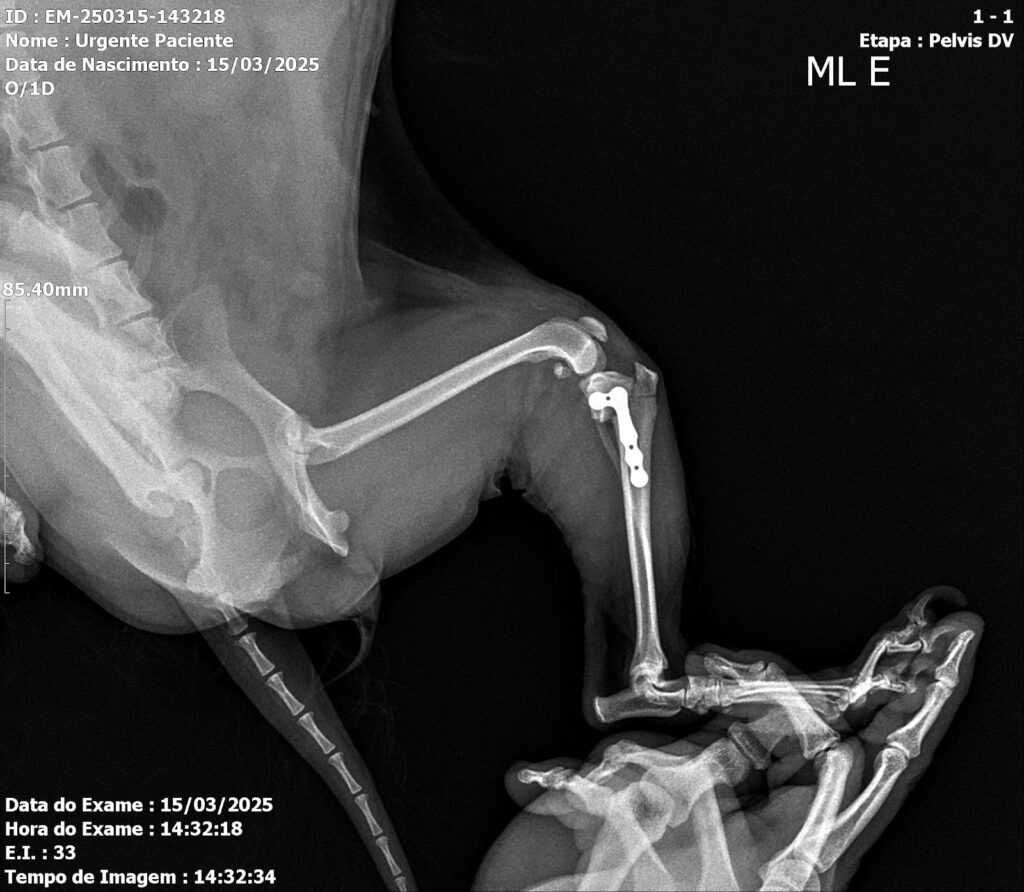
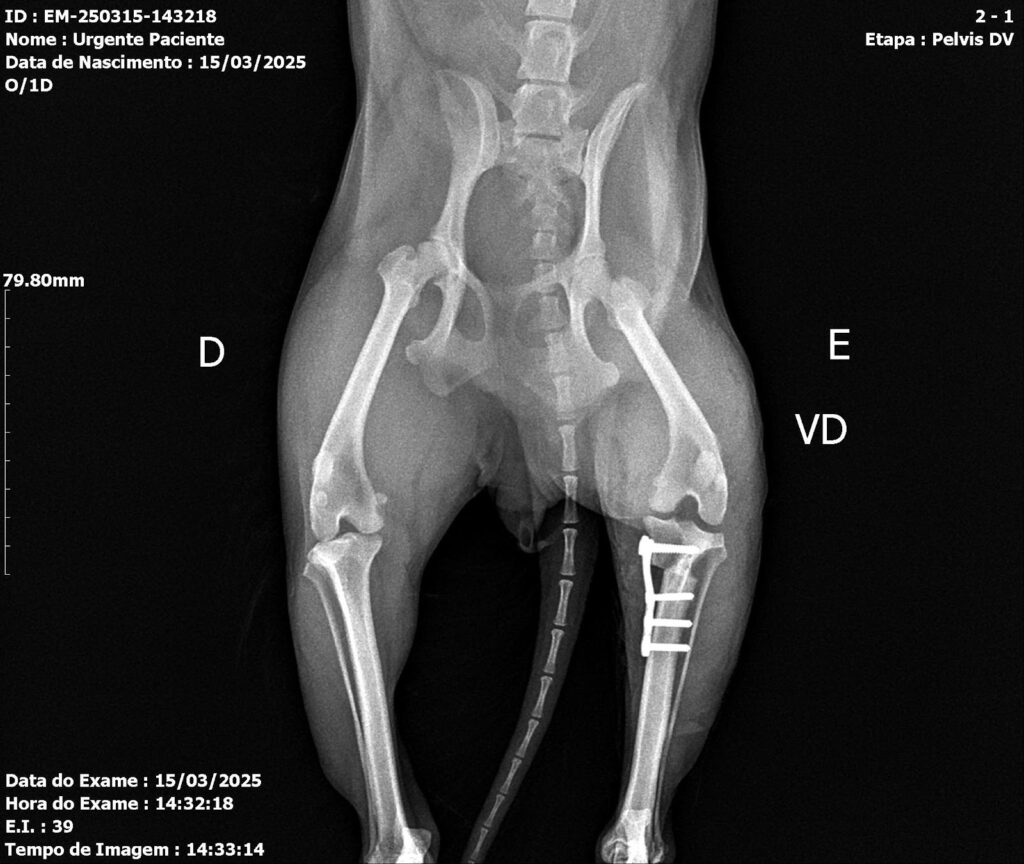
Postoperative evaluation included assessment of range of motion, limb alignment, and joint stability. Radiographs confirmed appropriate implant positioning and patellar alignment (Figures 4 and 5). A slight reduction of the medial femorotibial joint space was noted, with preservation of overall congruence. Mild lateral displacement of the patella was observed on the craniocaudal view and minimal caudal displacement on the mediolateral view. Increased soft-tissue opacity and volume, compatible with postoperative inflammatory changes, were also identified. The semicircular osteotomy in the proximal third of the left tibia and adequate implant positioning confirmed correct surgical execution.
Postoperative medication included metamizole (25 mg/kg, BID, 7 days), tramadol hydrochloride (4 mg/kg, BID, 7 days), and amoxicillin-clavulanate (25 mg/kg, BID, 10 days). After 48 hours, partial weight bearing was observed. At 21 days, full weight bearing was evident. At 30 days, occasional mild lameness persisted; however, by 60 days postoperatively, normal gait was restored without clinical abnormalities.
After 180 days, radiographic reevaluation showed the patella in its normal anatomical position, complete bone healing without evidence of fracture or osteotomy line, and normal tibial and femoral alignment.
Discussion
This report describes the concomitant occurrence of MPL and CCLD in a Yorkshire Terrier successfully treated with mTPLO combined with trochleoplasty. The findings suggest that this approach can effectively correct patellar luxation while restoring stifle stability and reducing lameness. Nevertheless, long-term follow-up is necessary to monitor clinical progression.
The coexistence of these two conditions has been explained by two main pathophysiological hypotheses. The first proposes that alterations in the extensor mechanism of the stifle — including the quadriceps, trochlear groove, patellar ligament, and tibial tuberosity — result in articular laxity predisposing to instability (Kowaleski et al., 2018). The second attributes the primary instability to CrCL rupture, which alters the Q angle and predisposes to luxation (Kaiser et al., 2021). In the present case, the concomitant occurrence of both disorders supports the interdependence of these alterations and underscores the complexity of their surgical management.
Several studies have demonstrated that patellar luxation is more common in small-breed dogs, occurring up to twelve times more frequently than in large breeds (Priester, 1972). Females are also more predisposed than males (Priester, 1972; Hayes et al., 1994; Alam et al., 2007; O’Neill et al., 2016; Bosio et al., 2017). The most commonly affected breeds include Poodle, Spitz, Yorkshire Terrier, Chihuahua, French Bulldog, Lhasa Apso, Cavalier King Charles Spaniel, Bichon Frisé, Pug, Bulldog, West Highland White Terrier, Jack Russell Terrier, and Shih Tzu (Alam et al., 2007; O’Neill et al., 2016; Arthurs, 2006; Bound et al., 2009). Therefore, the fact that the patient was a seven-year-old female Yorkshire Terrier corroborates the literature regarding breed, age, and sex predisposition.
Age is also a relevant factor, as dogs between five and seven years old are at greater risk for degenerative CrCL rupture (Spinella et al., 2021), consistent with the present case. Diagnosis of grade II patellar luxation was confirmed by positive cranial drawer and tibial compression tests and radiographic findings consistent with Singleton’s (1969) description.
The measured tibial plateau angle (118.4°) was essential for osteotomy planning, since this parameter directly influences CrCL biomechanical forces (Slocum & Devine, 1983). The modified TPLO, combined with trochleoplasty, aimed to simultaneously correct instability due to CrCL rupture and grade II patellar luxation, with reduced surgical aggressiveness and shorter operative time. Although TPLO is well established for CrCL rupture treatment, its application combined with patellar luxation management remains sparsely documented, emphasizing the relevance of this report.
Postoperative radiographic evaluation demonstrated adequate implant positioning and alignment, confirming the efficacy of the technique. The inflammatory changes observed were expected during the immediate postoperative phase. While short-term outcomes were satisfactory, complete functional recovery requires long-term follow-up to assess potential reluxation, complications, or degenerative progression.
Patellar luxation may be classified according to severity: grade I, manually luxatable and self-reducing; grade II, luxating during stifle flexion or manipulation and remaining luxated until stifle extension or manual repositioning; grade III, permanently luxated but manually reducible with immediate reluxation; and grade IV, permanently luxated and irreducible (Singleton, 1969).
Conclusion
This study demonstrates the feasibility and clinical efficacy of the mTPLO technique for the simultaneous treatment of CCLD and grade II MPL in a Yorkshire Terrier. Although this report describes a single case, the results indicate that the technique effectively restores patellar alignment and locomotor function, minimizing reluxation risk and avoiding major complications. Furthermore, this approach allows a reduced number of osteotomies, contributing to shorter surgical time and less postoperative discomfort.
Despite promising short-term results, long-term monitoring and larger sample studies are essential to confirm and validate these findings. Overall, the combined mTPLO approach represents a viable surgical alternative for the concurrent management of MPL and CCLD in small-breed dogs, improving prognosis and quality of life.
Figures 1 and 2: Preoperative radiographs of the right pelvic limb of a 7-year-old female Yorkshire Terrier. (A) Mediolateral projection showing medial patellar luxation (MPL) associated with cranial cruciate ligament disease. (B) Craniocaudal projection demonstrating misalignment and joint alterations consistent with the described orthopedic conditions.
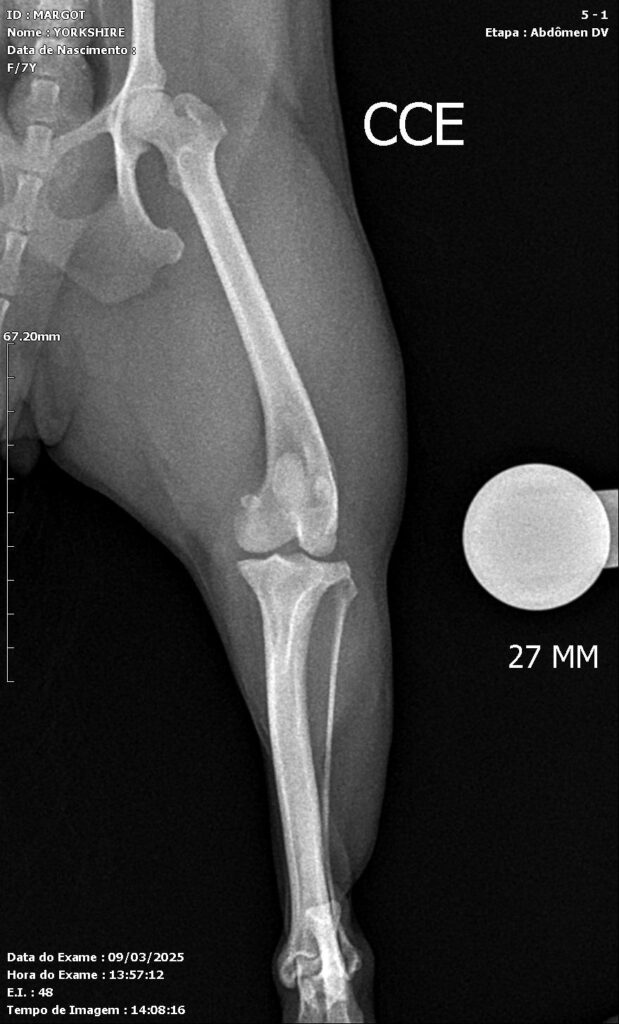
Figure 3: Preoperative surgical planning. Mediolateral projection showing the measurements, angles, and positioning of the fixation plate to be used during the procedure.
Figures 4 and 5: Ventrodorsal and mediolateral radiographs of the left pelvic limb in the immediate postoperative period, showing fracture stabilization using an orthopedic plate and screws, with proper bone alignment.
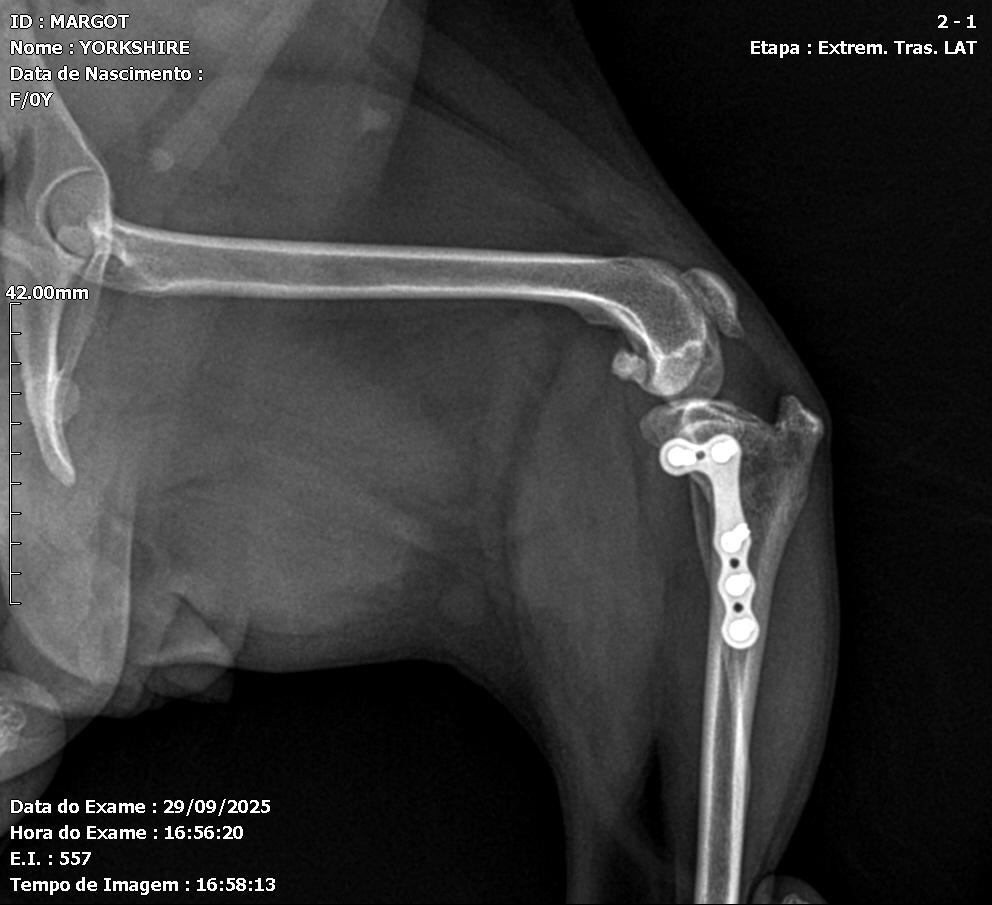
Figures 6 and 7: Lateral radiographic projections of the left pelvic limb, 180 days after the modified TPLO surgical procedure for simultaneous correction of medial patellar luxation and cranial cruciate ligament rupture. Adequate bone healing, maintenance of patellar alignment, and stable positioning of the orthopedic implants are observed, with no evidence of postoperative complications.

References
Alam, M. R., Lee, J. I., Kang, H. S., Kim, I. S., Park, S. Y., Lee, K. C., & Kim, N. S. (2007). Frequency and distribution of patellar luxation in dogs. Veterinary and Comparative Orthopaedics and Traumatology, 20(01), 59-64.
Alam, M. R., Lee, J. I., Kang, H. S., Kim, I. S., Park, S. Y., Lee, K. C., & Kim, N. S. (2007). Frequency and distribution of patellar luxation in dogs. Veterinary and Comparative Orthopaedics and Traumatology, 20(01), 59-64.
Arnoczky, S. P., & Marshall, J. L. (1977). The cruciate ligaments of the canine stifle: an anatomical and functional analysis. American journal of veterinary research, 38(11), 1807-1814.
Arthurs, G. I., & LANGLEY‐HOBBS, S. J. (2006). Complications associated with corrective surgery for patellar luxation in 109 dogs. Veterinary surgery, 35(6), 559-566.
Bosio, F., Bufalari, A., Peirone, B., Petazzoni, M., & Vezzoni, A. (2017). Prevalence, treatment and outcome of patellar luxation in dogs in Italy. Veterinary and Comparative Orthopaedics and Traumatology, 30(05), 364-370.
Bound, N., Zakai, D., Butterworth, S. J., & Pead, M. (2009). The prevalence of canine patellar luxation in three centres. Veterinary and Comparative Orthopaedics and Traumatology, 22(01), 32-37.
Brandt, K. D., Myers, S. L., Burr, D., & Albrecht, M. (1991). Osteoarthritic changes in canine articular cartilage, subchondral bone, and synovium fifty‐four months after transection of the anterior cruciate ligament. Arthritis & rheumatism, 34(12), 1560-1570.
Comerford, E. J., Smith, K., & Hayashi, K. (2011). Update on the aetiopathogenesis of canine cranial cruciate ligament disease. Veterinary and Comparative Orthopaedics and Traumatology, 24(02), 91-98.
Conzemius, M. G., Evans, R. B., Besancon, M. F., Gordon, W. J., Horstman, C. L., Hoefle, W. D., … & Wagner, S. D. (2005). Effect of surgical technique on limb function after surgery for rupture of the cranial cruciate ligament in dogs. Journal of the American Veterinary Medical Association, 226(2), 232-236.
Hayes, A. G., Boudrieau, R. J., & Hungerford, L. L. (1994). Frequency and distribution of medial and lateral patellar luxation in dogs: 124 cases (1982–1992). Journal of the American Veterinary Medical Association, 205(5), 716-720.
Kaiser, S., Cornely, D., Colder, W., Garner, M. T., Wolf, K. J., Waibl, H., & Brunnberg, L. (2001). The correlation of canine patellar luxation and the anteversion angle as measured using magnetic resonance images. Veterinary Radiology & Ultrasound, 42(2), 113-118.
Kowaleski, M. P., Boudrieau, R. J., Pozzi, A., Tobias, K. M., & Johnston, S. A. (2017). Stifle joint.
Livet, V., Taroni, M., Ferrand, F. X., Carozzo, C., Viguier, E., & Cachon, T. (2019). Modified triple tibial osteotomy for combined cranial cruciate ligament rupture, tibial deformities, or patellar luxation. Journal of the American Animal Hospital Association, 55(6), 291-300.
Marino, D. J., & Loughin, C. A. (2010). Diagnostic imaging of the canine stifle: a review. Veterinary surgery, 39(3), 284-295.
O’Neill, D. G., Meeson, R. L., Sheridan, A., Church, D. B., & Brodbelt, D. C. (2016). The epidemiology of patellar luxation in dogs attending primary-care veterinary practices in England. Canine genetics and epidemiology, 3(1), 4.
Priester, W. A. (1972). Sex, size, and breed as risk factors in canine patellar dislocation. Journal of the American Veterinary Medical Association, 160(5), 740-742.
Rafla, M., Yang, P., & Mostafa, A. (2025). Canine Cranial Cruciate Ligament Disease (CCLD): A Concise Review of the Recent Literature. Animals, 15(7), 1030.
Singleton, W. B. (1969). The surgical correction of stifle deformities in the dog. Journal of Small Animal Practice, 10(2), 59-69.
Slocum, B., & Slocum, T. D. (1993). Tibial plateau leveling osteotomy for repair of cranial cruciate ligament rupture in the canine. Veterinary Clinics of North America: Small Animal Practice, 23(4), 777-795.
Spinella, G., Arcamone, G., & Valentini, S. (2021). Cranial cruciate ligament rupture in dogs: review on biomechanics, etiopathogenetic factors and rehabilitation. Veterinary sciences, 8(9), 186.
Tashman, S., Anderst, W., Kolowich, P., Havstad, S., & Arnoczky, S. (2004). Kinematics of the ACL‐deficient canine knee during gait: serial changes over two years. Journal of orthopaedic research, 22(5), 931-941.
1 (https://orcid.org/0000-0003-1258-0623)
2 (https://orcid.org/0009-0001-0858-5272)
3 (https://orcid.org/0000-0003-0434-7549)