REGISTRO DOI: 10.69849/revistaft/ra10202004122238
Milena Raquel Charbel Dias Bonon
Abstract
Atopic dermatitis (AD) is a significant concern in pediatric health, affecting a large number of children globally and frequently continuing into adulthood. Characterized by itchy and inflamed skin, AD is not only a dermatological issue but is also linked to various allergic conditions, such as asthma and allergic rhinitis. The complexity of AD necessitates early recognition and effective management strategies to reduce the adverse effects on children’s quality of life and that of their families. Recent studies have focused on different aspects of AD, including its phenotypes and preventive measures like emollient and probiotic use. Although there is currently no definitive cure, treatment strategies aimed at restoring the skin barrier and controlling inflammation have shown encouraging results. These approaches emphasize the importance of maintaining skin hydration and addressing inflammatory responses, thereby helping to alleviate symptoms. Furthermore, research has highlighted the role of environmental factors and genetic predispositions in the development of AD and its associated comorbidities. As such, ongoing research into innovative therapies and preventive strategies is essential for improving care outcomes. The integration of current knowledge regarding AD, alongside practical preventive and treatment approaches, holds promise for enhancing the overall health and well-being of affected children and their families. This comprehensive understanding underscores the need for continued efforts in both research and clinical practice to tackle the challenges posed by atopic dermatitis.
Keywords: Atopic Dermatitis; Pediatric Health; Allergic Conditions; Skin Barrier; Preventive Strategies.
Atopic dermatitis (AD), often referred to as atopic eczema, is a chronic inflammatory skin condition that primarily affects children but can occur in individuals of any age. This condition is marked by intensely itchy, dry, red, and scaly skin lesions, commonly found in areas such as the folds of the arms, legs, face, and neck. Symptoms typically manifest in childhood and may either persist or improve as individuals age. A genetic predisposition and a family history of allergic conditions, such as asthma and allergic rhinitis, are commonly associated with AD, indicating a potential link between these diseases. Although the precise etiology of atopic dermatitis remains unclear, it is believed to arise from a combination of immunological factors, environmental influences, and a compromised skin barrier, which makes the skin of affected individuals more sensitive to irritants and allergens, leading to inflammation and discomfort.
In infants, the onset of AD is particularly prevalent, often surfacing within the first few months of life. The constant itching associated with this condition can disrupt sleep, and in more severe cases, scratching may lead to secondary infections. Effective management of atopic dermatitis focuses on restoring the skin barrier and mitigating inflammation. Common strategies include the regular application of moisturizers, use of topical corticosteroids during flare-ups, and avoidance of environmental triggers. Maintaining proper hygiene and ensuring a humid environment can also help in preventing skin dryness. Recently developed treatments, such as calcineurin inhibitors and biological therapies, are increasingly being utilized for moderate to severe cases.
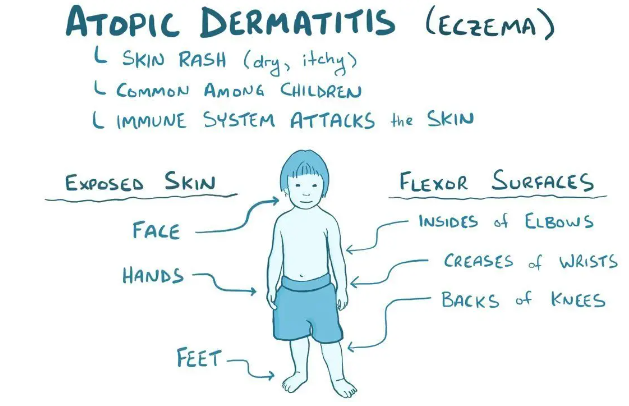
Figure 1: Common areas of occurrence of atopic dermatitis in children.
Source: Osmosis.
Although atopic dermatitis currently has no cure, symptoms can be managed through appropriate treatments and lifestyle changes, significantly enhancing the quality of life for both the affected child and their family.
The study by Roduit et al. (2017) aimed to categorize different phenotypes of atopic dermatitis in children based on the disease’s onset and progression until the age of six. Using latent class analysis, the researchers identified four groups: early-onset phenotypes (before two years), which included both transient and persistent types; a late-onset phenotype (after two years); and a group with rare or absent AD. The findings revealed that children exhibiting early-onset and persistent symptoms faced a notably higher risk of developing asthma and food allergies, underscoring the necessity for early identification to inform allergy prevention strategies.
Amat et al. (2018) explored the multifaceted nature of atopic dermatitis, emphasizing its various causes and developmental mechanisms that differ based on the age of onset, severity, ethnicity, treatment response, and triggers. The focus was on severe phenotypes characterized by early-onset AD and lifelong severity, frequently linked with allergic asthma and food allergies. The study posited that a defect in the epithelial barrier might be a principal factor in the development of allergic diseases, elucidating the progression from AD to allergic asthma. Additionally, they found that the severity of AD correlates with the risk of developing food allergies, and factors such as early and severe AD, male gender, parental history of asthma, and multiple sensitizations contribute to the atopic march. The authors advocated for environmental interventions and targeted therapies to restore skin barrier function, recommending the early application of emollients for children at high risk.
The research conducted by Perrett and Peters (2020) highlighted the widespread impact of atopic dermatitis, affecting approximately one-quarter of children globally, with rising prevalence and persistence into adulthood. Often beginning in early life, AD presents with dry, itchy, and scaly skin, leading to significant quality of life challenges along with social and financial burdens. The study examined the role of mutations in the filaggrin gene (FLG), which compromises the skin barrier and is associated with AD, food sensitization, and allergies. While earlier pilot studies suggested that regular emollient use could prevent AD by enhancing skin barrier function, two major trials—PreventADALL and another by Joanne Chalmers—did not find significant evidence that emollients or early complementary feeding could delay or prevent AD in infants. Despite these findings, the trials indicated a potential synergistic effect from combined interventions, although adherence to the protocols was low, necessitating further exploration of preventive strategies.
Finally, the study by Silverberg and Durán-McKinster (2017) identified atopic dermatitis as the leading cause of pediatric dermatology consultations in developed countries. Characterized by recurrent, itchy rashes in typical areas, it is often accompanied by a family or personal history of atopy, with most cases (85%) diagnosed by the age of five. Comorbidities based on age can significantly influence disease progression. While topical corticosteroids remain the mainstay of treatment, issues such as corticosteroid phobia and side effects can complicate their application. Alternatives like topical calcineurin inhibitors are effective for sensitive regions, while systemic treatments may include antihistamines, immunosuppressants, and phototherapy, tailored specifically for pediatric patients.
In addition, the research by Pyun (2014) examined atopic dermatitis as a common inflammatory allergic condition, especially prevalent in infancy, marked by pruritic skin lesions. It often represents the initial stage of the atopic march, with variable disease courses. Many children may experience resolution of AD symptoms as they grow, while others might develop respiratory allergies, including asthma and rhinoconjunctivitis. Cross-sectional and longitudinal studies from multiple countries have supported the notion of a natural progression of the disease. Young children, particularly those with genetic predispositions, are likely to experience more severe and persistent forms of AD. It is estimated that approximately 40%-70% of childhood AD cases resolve by ages six to seven, although more than half of these children may go on to develop respiratory allergies in later childhood.
Jiang et al. (2020) conducted an updated meta-analysis examining the effectiveness of probiotics in preventing and treating atopic dermatitis in children, alongside understanding their clinical role in AD interventions. Analyzing 25 studies from various databases, including prevention studies involving 3,049 children and treatment studies with 816 participants, the meta-analysis indicated that probiotics significantly reduced the incidence of AD, especially when using mixed strains. Moreover, interventions directed at both pregnant mothers and their infants yielded more effective results. Extended treatment durations of over six months correlated with a notable decline in both the incidence and symptom severity of AD, as evidenced by improvements in the Scoring Atopic Dermatitis (SCORAD) index. However, it was also noted that probiotics given exclusively to infants might lead to negative preventive outcomes, warranting caution due to the moderate heterogeneity among the studies and insignificant subgroup differences, indicating the need for more robust randomized controlled trials to assess the long-term effects of probiotics on atopic dermatitis.
Atopic dermatitis (AD) represents a significant challenge in pediatric health, affecting a considerable proportion of children worldwide and often persisting into adulthood. Evidence highlights the complexity of this condition, which not only manifests as pruritic skin lesions but is also closely associated with a variety of allergic diseases, such as asthma and allergic rhinitis. Early recognition and effective management of AD are crucial for mitigating the negative impacts on the quality of life of affected children and their families. Recent studies have explored various aspects of atopic dermatitis, from disease phenotypes to preventive interventions, including the use of emollients and probiotics.
While the lack of a definitive cure makes a multifaceted approach essential, treatment strategies aimed at restoring the skin barrier and controlling inflammation have shown promising efficacy. Research also underscores the importance of environmental interventions and the role of genetics in the predisposition to AD and its comorbidities. Finally, continued research, especially regarding innovative therapies and preventive methods, is vital for enhancing care and quality of life for children affected by this challenging condition. The integration of knowledge about atopic dermatitis, combined with practical approaches in prevention and treatment, could contribute to a healthier future for young patients and their families.
References
Amat, F., Amat, F., Soria, A., Soria, A., Tallon, P., Bourgoin-Heck, M., Lambert, N., Deschildre, A., Just, J., & Just, J. (2018). New insights into the phenotypes of atopic dermatitis linked with allergies and asthma in children: An overview. Clinical & Experimental Allergy, 48, 919 – 934. https://doi.org/10.1111/cea.13156.
Jiang, W., Ni, B., Liu, Z., Liu, X., Xie, W., Wu, I., & Li, X. (2020). The Role of Probiotics in the Prevention and Treatment of Atopic Dermatitis in Children: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials. Pediatric Drugs, 22, 535 – 549. https://doi.org/10.1007/s40272-020-00410-6.
Osmosis. Atopic dermatites. Available in: https://www.osmosis.org/learn/atopic_dermatitis (accessed 26 September 2024).
Perrett, K., & Peters, R. (2020). Emollients for prevention of atopic dermatitis in infancy. Lancet. https://doi.org/10.1016/S0140-6736(19)33174-5.
Pyun, B. (2014). Natural History and Risk Factors of Atopic Dermatitis in Children. Allergy, Asthma & Immunology Research, 7, 101 – 105. https://doi.org/10.4168/aair.2015.7.2.101.
Roduit, C., Frei, R., Depner, M., Karvonen, A., Renz, H., Braun‐Fahrländer, C., Schmausser-Hechfellner, E., Pekkanen, J., Riedler, J., Dalphin, J., Mutius, E., Lauener, R., Hyvärinen, A., Kirjavainen, P., Remes, S., Roponen, M., Dalphin, M., Kaulek, V., Ege, M., Genuneit, J., Illi, S., Kabesch, M., Schaub, B., Pfefferle, P., & Doekes, G. (2017). Phenotypes of Atopic Dermatitis Depending on the Timing of Onset and Progression in Childhood. JAMA Pediatrics, 171, 655–662. https://doi.org/10.1001/jamapediatrics.2017.0556.
Silverberg, N., & Durán-McKinster, C. (2017). Special Considerations for Therapy of Pediatric Atopic Dermatitis.. Dermatologic clinics, 35 3, 351-363 . https://doi.org/10.1016/j.det.2017.02.008.