REGISTRO DOI: 10.5281/zenodo.7118120
Authors:
1Henrique Bosio Zemel
Dionei Freitas de Morais
Matheus Rodrigo Laurenti
Carlos Eduardo Dall Aglio Rocha
1Department of Neurosurgery, Hospital de Base de São José do Rio Preto
E-mail: henriquebz@terra.com.br
ABSTRACT
Background: Metastasis to the brain represents an uncommon and severe complication of endometrial carcinoma, and the presence of a single brain methastasis with no other evidence of sistemic disease is extremely rare, with few relates in literature.
Case report: A 82 year-old women with treatment of an uterine endometrial carcinoma performed 16 months prior was suffering fron haedache and seizures for 3 weeks. MRI scan demonstrating an enhancing lesion in the right parietal lobe. The patient underwent a right-parietal craniotomy with complete removal. Histologic examination showed an adenocarcinoma compatible with endometrial primary tumor. The patient was discharged 4 days after the surgery and referred for oncologic follow-up and radiotherapy.
Conclusion: Solitary Metastasis to the brain of endometrial carcinoma with no other evidence of sistemic disease is rare and suggest a better prognosis. In these group of patients, complete surgical resection of the metastasis followed by whole-brain radiotherapy potentially can improve survival. Further studies should clarify treatment-related morbidity and the role of chemotherapy and radiosurgery to the therapeutic plan of these patients.
Keywords: Endometrial carcinoma; Metastasis; Single lesion.
INTRODUCTION
It is estimated that between 10% and 30% of all patients with cancer develop brain metastasis.(1) The majority of brain metastases arise from lung, breast or skin primary sites(5). Brain metastasis from endometrial carcinoma(EC) is extremely uncommon and, general, are associated with widespread dissemination in the course of disease.The ain of this paper is describe a case of a patient with a single brain methastasis from EC, wich no other evidence of sistemic desease. A rare case with few relates in literature.
CASE REPORT
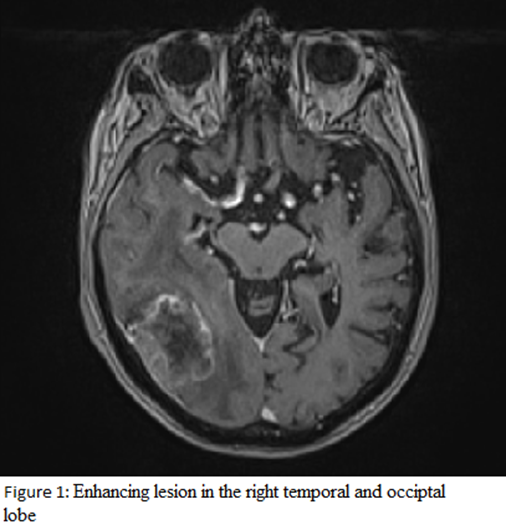
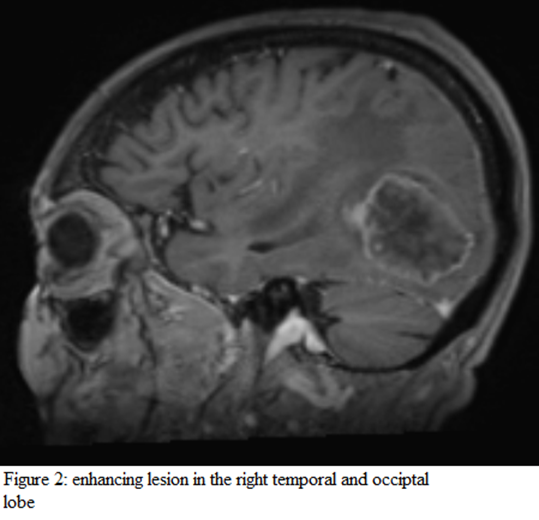
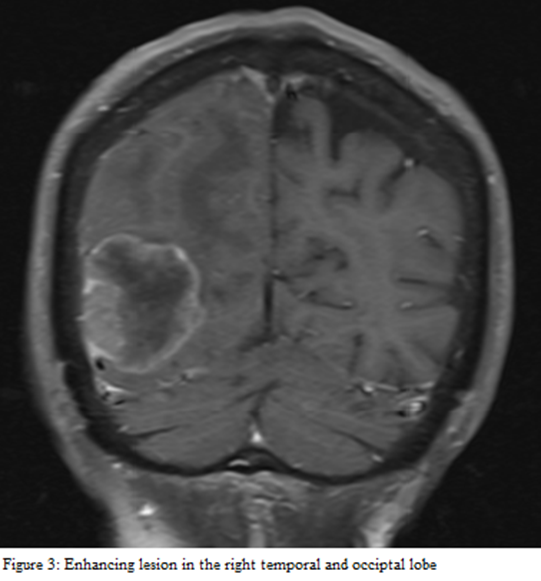
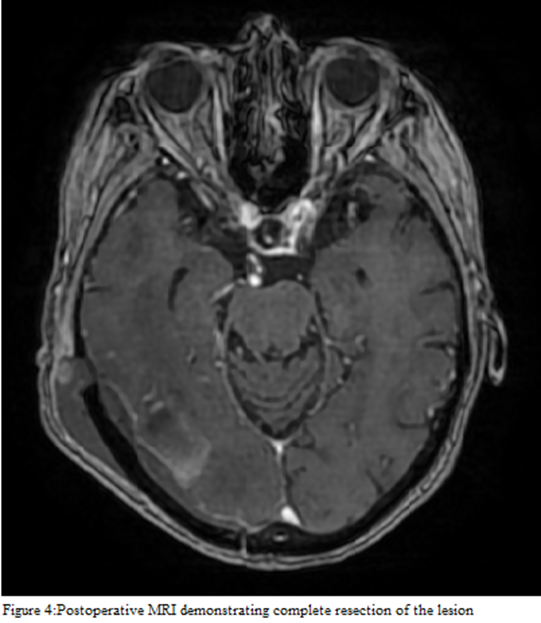
A 82 year-old women was suffering from headache and seizures for 3 weeks. The patient medical history was significant for a treatment of an uterine endometrial carcinoma performed 16 months prior. At the time of diagnosis of uterine neoplasm was not evidence of distant metastasis. Endometrioid carcinoma was treated with surgery and radiotherapy. MRI scan with Gd-DPTA was obtained demonstrating an enhancing lesion in the right temporal and occiptal lobe (Figures 1,2,3). A complete metastatic work-up (total-body CT and osseous scintigraphy) did not reveal a primary focus nor any other metastatic lesions. The patient underwent a right-parietal craniotomy. The tumor had a well-defined cleavage plane allowing a complete removal. Histologic examination showed an adenocarcinoma compatible with endometrial primary tumor. Postoperative MRI confirmed complete resection of the lesion(Figure 4). The patient was discharged 4 days after the surgery and referred for oncologic follow-up and radiotherapy.
DISCUSSION
The prevalence of brain metastases in women with endometrial cancer variety between 0.3-0,9%(4). Many authors have reported that brain metastasis in endometrial cancer is usually found in association with widespread disseminated disease. In contrast, our case report described a patient who did not have systemic disease at the time of diagnosis of her brain metastasis, which increases the rarity of the case.(4) Clinical manifestation of brain metastasis included headache (80%), motor weakness (50%), seizures (20%), confusion (10%), balance (10%), and visual disturbances (10%).(3) Studies confirms that patients with endometrial cancer diagnosed with cerebral metastases have a life expectancy of approximately 6.5 months after the detection of central nervous system involvement. The few cases of solitary brain metastasis from uterine carcinoma described until now in the literature precludes to draw conclusions about the optimal therapeutic management of these patients. However, surgical removal followed by whole brain radiotherapy proved to be a good option in patients with brain metastases in presence of control of systemic disease and can improve the patients’ prognosis. (5) The role of chemotherapy in the management of CNS metastases remains unclear. Stereotactic radiosurgery may be effective in treating patients with metastasis smaller than 3 cm . When metastasis is not amenable to surgical excision, stereotactic biopsy could be an effective diagnostic modality.(5)
CONCLUSION
Metastasis to the brain represents an uncommon and severe complication of endometrial carcinoma, and the presence of a single brain methastasis with no other evidence of sistemic disease is extremely rare, with few relates in literature. The presence of an solitary lesion in the brain and the absence of extracerebral spread suggest a better prognosis. In these group of patients, a treatment plan that includes complete surgical resection of the metastasis followed by whole-brain radiotherapy potentially can improve survival. Further studies should clarify treatment-related morbidity, the role of radiosurgery, and the possible implications of adding chemotherapy to the therapeutic plan of these patients.
IMAGES
REFERENCES
1. BEUCLER, N. et al. Brain metastases in endometrial cancer: A systematic review of the surgical prognostic factors. European journal of obstetrics, gynecology, and reproductive biology, v. 258, p. 240–252, 2021.
2. BHAMBHVANI, H. P. et al. Brain metastases from endometrial cancer: Clinical characteristics, outcomes, and review of the literature. World neurosurgery, v. 147, p. e32–e39, 2021.
3. CORMIO, G. et al. Brain metastases from endometrial carcinoma. Gynecologic oncology, v. 61, n. 1, p. 40–43, 1996.
4. GIEN, L. T. et al. Brain metastases from endometrial carcinoma: a retrospective study. Gynecologic oncology, v. 93, n. 2, p. 524–528, 2004.
5. SALVATI, M. et al. Solitary brain metastases from uterus carcinoma: Report of three cases. Journal of neuro-oncology, v. 66, n. 1/2, p. 175–178, 2004.
6. UCCELLA, S. et al. Primary brain metastases of endometrial cancer: A report of 18 cases and review of the literature. Gynecologic oncology, v. 142, n. 1, p. 70–75, 2016.