REGISTRO DOI: 10.69849/revistaft/ma10202408220722
Márcia Silvério Cabral Maia1
Maria Aparecida dos Santos Dourado Dares1
Adriane Viapiana Bossa2
Angela Mara Rambo Martini2
Jefferson Souza Santos3
ABSTRACT
Male hypogonadism represents a decrease in testicular function with low testosterone production and infertility affecting men from the age of 35-40. It leads to symptoms as loss of libido, loss of muscle strength, and depression. Medicinal Biomagnetism is a non-invasive integrative therapy based on the use of static magnetic fields generated by magnets that correct pH distortions. The aim of this study is to present a Medicinal Biomagnetism (MB) Protocol for adjuvant treatment in cases of Male Hypogonadism. This study is based in a descriptive-qualitative literature review of an exploratory nature conducted in the journal databases of SciELO, Google Scholar, PubMed, MB books, and Par Magnético Institute (IPM) course material. The MB systematic protocol was presented to be applied by healthcare professionals as adjuvant treatment for male hypogonadism seeking to minimize or eliminate the causes and symptoms generated by the dysfunction. Therefore, the studies evaluating this technique and the specific protocol are necessary due to low cost, minimal contraindications, and great therapeutic potential of the MB.
Keywords: Medicinal Biomagnetism; Biomagnetic Pair; Magnetic Therapy; Male Hypogonadism; Magnet; Magnets; Static Magnetic Fields; Complementary Therapies.
INTRODUCTION
Male hypogonadism or androgen deficiency is characterized by a decline in plasma testosterone in men. It is commonly associated with factors related to changes in hypothalamic central and upper regions of the brain that affects peripheral organs, testes, and adrenal glands (MELO et al., 2013; JUNIOR et al., 2021).
The production of the main sex hormone, testosterone, is regulated through two pituitary hormones: luteinizing hormone (LH) and follicle-stimulating hormone (FSH). The complexity of the hypothalamic-pituitary-gonadal axis relationship means that since small alterations in any of the sexual hormones have the potential to impact in the gonadotropic axis, leading to a hypogonadism state (MATOS, MOREIRA, and GUEDES, 2003).
In the United States, there is a prevalence of 4-5 million hypogonadal individuals in a population of 40 million elderly people (CALIXTO, 2021). The disease affects men from 35 to 40 years old and is evidenced by symptoms such as loss of libido or sexual desire, decreased muscle mass with decreased muscle strength, loss of energy, depression, and erectile dysfunction (ROHDEN, 2011; MARTITS and COSTA, 2004).
The characteristic signs and symptoms of male hypogonadism are characterized by an increase in fibrous muscular tissue and total adipose tissue, fat redistribution, osteopenia, osteoporosis, and decreased testicular volume (MELO et al., 2013).
The Androgen Deficiency in the Aging Male (ADAM) questionnaire is also a reasonable screening tool to detect androgen deficiency in men with low testosterone above 40 years old, as well as a potential instrument to rule out hypogonadism. Among the ten symptoms commonly observed in this questionnaire and used to develop it, some stand out, such as fatigue, irritability, depression, and decreased sexual interest (LOPEZ, 2022; MARTITS and COSTA, 2004).
Low testosterone levels may occur due to three factors. In primary hypogonadism, the testes stop producing sperm, testosterone, or both, which may be related to some basic mechanisms such as intrinsic testicular damage. Secondary hypogonadism is an anomaly in the hypothalamic-pituitary axis due to decreased androgens or organ absence (JUBIZ and CRUZ, 2007). In the third factor, the environmental is characterized by the third factor involving all of these three mechanisms. The first occurs in men with normal gonadal function but whose serum testosterone concentrations are modified due to exposure to toxins, radiation, and microorganisms. The second behavioral mechanism is related to alcoholism, smoking, and hallucinogen use. The last, the socio-economic mechanism is associated with malnutrition, stress, and the presence of chronic diseases (LOPEZ, 2022).
The clinical diagnosis of male hypogonadism is biochemically made through testosterone measurement. This is evaluated through laboratory early and aging measurements associated with alterations in the endocrine system. Such alterations may be characterized as a decrease in growth hormone secretion and in LH and FSH release patterns. Moreover, it may cause a decrease in sex hormone levels that ultimately lead to androgen deficiency (JUNIOR et al., 2021).
The treatment of male hypogonadism is performed with hormone replacement therapy which aims to restore serum testosterone levels. However, in many cases, replacement therapy does not solve the genesis of the problem, and it is necessary to continue its use (MOLLE et al., 2004). Therefore, there is a need for new therapeutic interventions to find and treat the cause of the dysfunction, and therefore, Medicinal Biomagnetism may be a promising adjunctive option.
Medicinal Biomagnetism (MB) is a therapy created by the Mexican Isaac Goiz Durán in 1988, based on the studies of Richard Broeringmeyer. This method detects, classifies, measures, and corrects the fundamental alterations of the pH in living organism correcting bioelectromagnetic distortions. These alterations may accumulate and combine to allow the development of symptoms, syndromes, and other health conditions (DURÁN, 2008; BROERINGMEYER, 1991). Durán continued to study and develop the therapeutic system of MB, which, after more than 30 years of its application resulted in a protocol for scanning the entire organism. This protocol, called the Complete Scanning (CS) has the ability to locate regions with bioelectromagnetic dysfunction and treat them through the application of Static Magnetic Fields (SMF) (DURÁN, 2008; MARTÍNEZ, 2018; BOSSA, 2021a).
The SMF used for MB treatment are generated by medium-intensity magnets ranging from approximately 1000 to 7500 Gauss. These are applied to specific regions of the body which may coincide with locations where signs and symptoms of diseases generated by biological, biochemical, or electrochemical dysfunctions, and even microorganisms occur (DURÁN, 2008).
The elementary characteristic of a magnet is the presence of SMF associated with two poles which may be natural or artificial, permanent or temporary (TANO and SILVÉRIO-LOPES, 2013; BROERINGMEYER, 1991). The most commonly used magnets in this technique are ferrite and neodymium magnets. The magnets are applied to points of bioelectromagnetic dysfunction generated by the polarization of H+ and OH- charges or other free radicals that remain in magnetic resonance with each other (MARTÍNEZ, 2018).
For Medicinal Biomagnetism, certain nomenclatures are used to differentiate the poles of the magnets. The North Biomagnetic Pole (negative) is described as sedative and anti-inflammatory. It is generated by the deficit of H+ with the presence of complex free radicals with negative polarity (OH-) where the pH is more alkaline than physiological levels; it may result in the presence and development of bacteria and parasites. The South Biomagnetic Pole (positive) has a stimulating and toning biological effect resulting from an excess of H+, acidifying the region, which may lead to the presence of viruses and fungi (DURÁN, 2008; BROERINGMEYER, 1991). These alterations occur due to changes in temperature leading to pH alterations. The points with alterations are the regions where the magnets will be impacted and are called Biomagnetic Pairs (BMP) (DURÁN, 2017).
The BMP is a set of charges that identify pathologies. Their interaction presents the same magnetic field, the same number of particles, the same frequency, separated and maintained by a natural dielectric generating energetic stability in the BMP. The induction of charges neutralizes pathogenic or dysfunctional bioenergetic distortions causing a resonance of the fields that leads the organism to a natural homeostasis, thus promoting health (DURÁN, 2014; MASA et al., 2019; FRANK, 2017).
The therapeutic system of MB considers the bioelectromagnetic origin of diseases, in addition to symptoms. It is a new therapeutic discipline that seeks the bioenergetic balance of organisms aiming for the Normal Energy Level (NEL), or homeostasis. It acts on metabolic and cellular processes correcting physiological, biochemical, immunological, and psychological alterations that must be kept under normal conditions (DURÁN, 2008; BROERINGMEYER, 1991; MASA et al., 2019).
MB is a painless technique with minimal side effects and contraindications. Attention should be paid to patients with pacemakers, pregnant women, especially during the first three months of gestation, and hemodynamically unstable patients (MARTÍNEZ, 2018).
The full MB scanning is carried out through kinesiology, a therapeutic discipline that uses a muscular test as a feedback system of the information stored in the subconscious, through the limbic system (Figure 1). In this system, the response to stress will be produced by the application of SMF produced by magnets resulting in the shortening of the right hemibody (GOIZ DURÁN, 2008; FRANK, 2017; PARRA, 2020).
Figure 1: kinesiology in MB
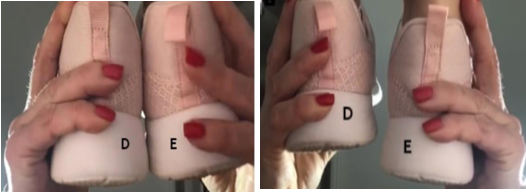
Source: Bossa (2021)
Starting from the application of the Complete MB Scanning consisting in the physical examination gives the possibility to report BMP. Thus, in front of the characteristic signals and symptoms of pathologies, specific protocols may be developed. The protocols complement the CS and assist the management of the MB treatment facilitating their application and approach within each pathology. This tends to enhance the effect of CS in the medium and long-term allowing for a reduction in the number of necessary treatments (MARTÍNEZ, 2017a; 2017b; BOSSA, 2021a).
The literature shows the relationship of health care protocols, care, assistance, monitoring, and evaluation with priority for therapeutic preventive activities and the development of best practices in health work processes (WERNECK et al., 2009; PAIM, 2004).
The development of MB protocols enables and facilitates the production of scientific knowledge in various organic dysfunctions in the field of MB. The treatment of male hypogonadism is performed with hormone replacement therapy aimed at restoring testosterone levels. In addition, there is a need for new therapeutic interventions that find and treat the cause of the dysfunction. Thus, the treatment with MB protocols may be a promising adjunctive option. Therefore, the aim of this study is to present a protocol of Medicinal Biomagnetism for the treatment and prevention of Male Hypogonadism.
MATERIALS AND METHODS
This study employed a descriptive bibliographic review as a method of inquiry with the aim of understanding a phenomenon without modifying it in order to comprehend the object of interest within a specific space and time (CARDOSO et al., 2005). Additionally, a qualitative approach was employed which complexly and interconnectedly evaluates concepts and hypotheses arising from various disciplines and areas of knowledge, engaging the observer in the world of interpretive practices (LOPES et al., 2008). This study was exploratory in nature and aimed to provide an approximate overview of a particular phenomenon seeking to better understand the identified phenomena to clarify concepts and raising propositions (CAMPOS and DIAS, 2012).
The review was conducted using the following journal databases: Scielo, Google Scholar, and PubMed. The search terms included: Male Hypogonadism, Medicinal Biomagnetism, Biomagnetic Pair Therapy, Magnetic Therapy, Magnets, Static Magnetic Fields, and Complementary Therapies. Studies published in English, Spanish, and Portuguese from 1989 to 2022 were included. In addition, only full articles related to male hypogonadism in adults with or without DOI were included. Paid articles, dissertations, repeated studies those related to female hypogonadism, tumor or congenital factors, and those that did not focus on endocrine dysfunction or signs and symptoms were excluded (Figure 2).
Regarding the topic of Medicinal Biomagnetism, books and theses by authors of the technique including course materials from the Par Magnético Institute (IPM) were used due to the scarcity of articles in this field (BOSSA, 2021c).
After conducting the methodological search, books, articles, and tables were read and translated analyzing symptoms of Male Hypogonadism related to hormonal, glandular, and functional problems and assessing whether these symptoms were related to the interventions described by Biomagnetic Pair Therapy. The results were grouped according to the subject; the research scenario and methodology were based on Biomagnetic Pair Therapy protocols focusing on the types of detoxification, dysfunctional, and special pairs considered the basis for developing the Protocol for the Treatment of Male Hypogonadism.
Figure 2: Descriptors

RESULTS
Following the search, 35 articles were identified in Scielo, 1180 in Google Scholar, 96 in PubMed, and 13 studies were to the themes of Medicinal Biomagnetism, Magnetic Therapy, Magnet, Magnets, and Static Magnetic Fields.
Among Durán books, four were found, namely “El Par Biomagnético” (2008 and 2017), “Fisiopatologia Biomagnética” (2014), “El Código Patógeno” (2010), and five handouts of attendance protocols related to Medicinal Biomagnetism from the Par Magnético Institute (IPM) by Bossa. These included “Protocolo de Rastreio do Biomagnetismo Medicinal” (2021a and 2021b) which presents the methods of applying therapy; “Biomagnetismo Medicinal Avançado” (2021c), referring to the protocols; “Apostila do Biomagnetismo Medicinal” (2021d); “Descrição dos Pares Biomagnéticos” (2019); three handouts by Martínez, “Guia de Pares Biomagnéticos Primer Nivel” (2017a) and “Segundo Nivel” (2017b), and “Manual del Biomagnetista” (2018); one thesis by Parra (2020), and one article with DOI by Frank (2017).
A total of 151 references were found including books and scientific articles. After selection, 48 references were included for the final use, as they met the established inclusion criteria, while 103 references were excluded as they were not relevant to this study; they did not provide pertinent information for the review relating the impact of male hypogonadism.
The MB protocols were developed by David Martínez (2017a and 2017b) and Isaac Goiz Dúran through clinical experience, as well as that of several Biomagnetism Therapists who repeated pairs for certain pathologies elaborating protocols to complement the effect of MB attendance.
Based on the studies about the relationship between hypogonadism and Medicinal Biomagnetism were possible to evaluate the potential of each BMP to act on the bioelectrical dysfunctions related to these same signs and symptoms. For a better understanding and visualization of this study and the method of applying MB, a treatment protocol flowchart for hypogonadism BMP was developed, as described in Figure 3.
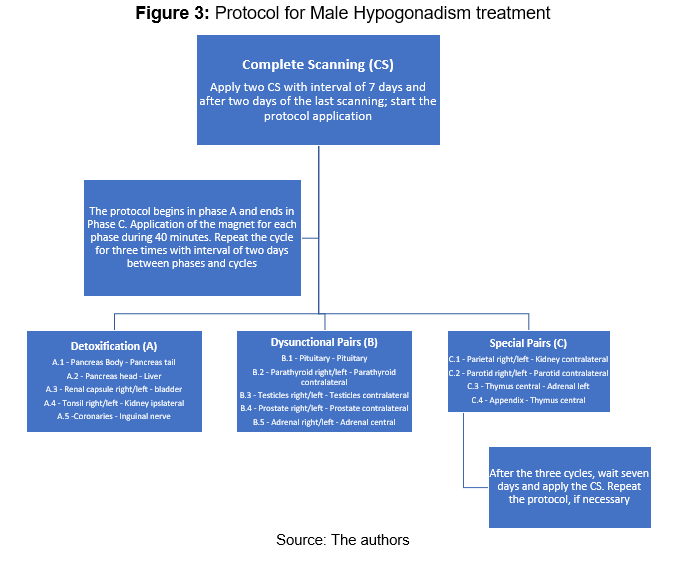
The Protocol for Male Hypogonadism consists initially of the application of two complete scanning with a seven-day interval between them. After the second scanning, a two-day interval is given. The first cycle is initiated corresponding to phases A (Detoxification), B (Dysfunctional), and C (Special Pairs), respecting this sequence with intervals of two days between each phase. The application of the magnet must be 40 minutes.
For the application of each cycle, Phase A corresponds to the impact of BMP A.1; A.2; A.3; A.4; and A.5. Phase B corresponds to BMP B.1; B.2; B.3; B.4; and B.5. In Phase C, C.1; C.2; C.3; and C.4 are impacted. This procedure must be repeated two more times maintaining the same two-day interval between them.
After the completion of the third cycle, a seven-day wait is required, followed by a new Complete Scanning. If necessary, the protocol is repeated, and if not, the therapy is discontinued. The repetition of the Male Hypogonadism Protocol depends on the biological individuality of each patient and should be evaluated according to the presence of BMP found in the last Complete Scanning.
DISCUSSION
This protocol was developed to optimize the effect of Complete Scanning (CS) in Medicinal Biomagnetism (MB). The proposed time interval between scanning is necessary due to the entropic alteration that may occur after each session. Adherence to this therapeutic pause is advised by Martínez (2018). The author also mentions the possibility of pathogens acquiring magnetic resistance. A distant comparison may be made to super microorganisms that develop resistance to antibiotics when used incorrectly. It should be noted that this is just a theory, a hypothesis that needs to be investigated, since studies that evaluated the biological effects of SMF related to infections using the same characteristics employed in MB have not been found. The existing studies use different magnitudes of magnetic field. It is worth noting that in MB this is only possible in the so-called Regular Pairs and Reservoir Pairs, not addressed in the cycles, but present in CS. Until conclusive studies are conducted on this matter, it is recommended to maintain a therapeutic precaution by adhering to the indicated time interval between complete scanning.
Regarding the cycles, the indicated interval between the applications of SMF is two days. The pairs involved in the cycles consist of Detoxification, Dysfunctional, and Special Pairs that aim only to stimulate specific tissues modulating the functioning of various glands and organs. It is believed that this allows greater functional effectiveness for detoxification organs. For glandular pairs, the action is the same, modulating glandular functioning. Meanwhile, the special pairs normalize the activity of important regions that directly or indirectly integrate organic systems (DURÁN, 2008; MARTÍNEZ, 2018; BROERINGMEYER, 1991).
The two-day interval between phases A, B, and C is indicated in this protocol to optimize patient care without requiring their daily availability in the clinic. A higher frequency could make it difficult for them to attend making the treatment unfeasible (MARTÍNEZ, 2018). The indicated time for the application of SMF should be 40 minutes per session including the duration of the 52 days of the treatment. In conventional medicine, the diagnosis of male hypogonadism is based on clinical symptoms and biochemical parameters of free testosterone; thus, the main treatment indication is hormonal replacement therapy (MOLLE et al., 2004). Medicinal Biomagnetism, as an Integrative and Complementary Therapy, may be an important tool as an adjuvant and supportive treatment to conventional medicine. According to Durán (2014), by identifying and correcting alterations through the use of SMF, it is possible to normalize organic function especially glandular function that modulates hormone production and secretion.
The human body naturally detoxifies organs; however, modern lifestyle has been generating an increasing amount of toxic residues at a faster pace, some of them called endocrine disruptors/regulators/interferers which can affect hormonal balance (GONÇALVES and CESTARZYCHAR, 2019). The treatment for Male Hypogonadism in Phase A is composed of Detoxification Pairs. The purpose of this phase is to enhance the natural detoxification of the body resulting in the elimination of residues and toxins to contribute to the strengthening of the immune system and efficiency of the other systems (SILVA, 2020; PEREIRA and CARDOSO, 2012).
Figure 5: Treatment Protocol – Phase A
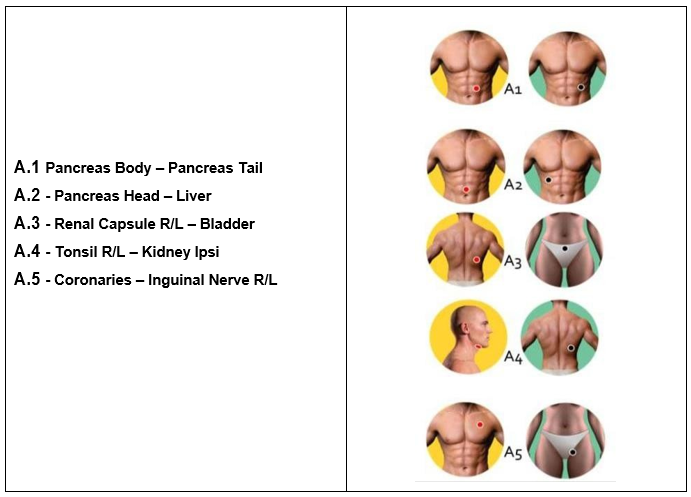
Source: The authors
According to the descriptions left by Durán (2014), the application of magnets to the pancreas aids in the process of heavy metal detoxification, digestive intoxication, central nervous system disorders, and digestive disorders (MARTÍNEZ, 2018; BOSSA, 2021b). The pancreas is both an endocrine and exocrine gland that produces important hormones, including insulin, glucagon, and somatostatin. In addition, its exocrine function secretes pancreatic juice containing digestive enzymes that pass into the small intestine (DELATTRE, 2004). Dellazari et al. (2010) describe that the main route of contamination of endocrine disruptors for humans is through agricultural foods with agrochemical or additive contaminants and contaminated water. Intoxication may affect the fetus even in the mother’s womb. Endocrine system dysfunctions caused by hormonal disruptors may affect interrelated systems, such as the immune system.
Regarding BMP A.2, Durán (2014) describes that the liver is also a detoxification organ for heavy metals such as mercury, lead, aluminum, and other metals. These are caused by the accumulation of oxidative products in cellular metabolism or the action of toxic chemicals. Carvalho et al. (2013) corroborate that biotransformation activities in the liver are associated with detoxification which may be a major problem because the effects of metabolites that may be highly reactive and toxic resulting in oxidative stress. The liver plays a central role in metabolism, as it receives nutrients and xenobiotics that are absorbed, transformed, stored, and released into the blood for elimination. Thus, the application of SMF over this organ could aid in the process of eliminating these toxins helping the body to recover the balance. Indirectly, this could improve the hypogonadism condition via integration of organic systems.
BMP A.3 would be the most important for promoting the elimination of waste from the body of individuals with hypogonadism, low glandular activity, and metabolic dysfunctions followed by electrochemical dysfunctions. In his book “Bioenergetic Pathophysiology,” Durán (2014) discusses the importance of the kidneys in the body’s detoxification process via toxin elimination. The renal capsule is a fibrous membrane closely attached to the renal surface. This is the protagonist of homeostasis by maintaining the internal environment and ensuring a physiological environment to assure the functionality of renal cells (BERNARD, 2021).
The bladder is an organ of the urinary system that functions to store urine produced in the kidneys. This reaches the bladder through the ureters and exits via the urethra eliminating metabolites previously existing in the bloodstream and filtered by the kidneys. The bladder performs functions of electrolytic regulation, hormonal production, and regulation of pressure levels for the maintenance of physiological homeostasis (MAGALHÃES et al., 2020). Lopez (2022) states that male hypogonadism could be due to various environmental factors such as exposure to toxins, radiation, microorganism residues, as well as behavioral factors such as alcoholism, smoking, and the use of hallucinogens. In addition, socioeconomic factors such as nutrition and stress may lead to transient modification of testosterone serum concentrations in the blood. Therefore, the choice of BMP A.3 is justified as a treatment.
According to the theory of Durán (2008), the BMP A.4 assists in the process of elimination of endotoxins and exotoxins. These are substances released from the body during the elimination of certain bacteria. The effect of the application of this BMP is to support the immune system (lymphocytes) whose function is to combat bacteria and infectious agents. According to Marinho (2010), the tonsils are two organs located at the back of the throat and are part of the body’s defense system functioning as the first barrier against microorganisms that invade the mouth. The Kidney is toned by the action of the south pole of the magnet enhancing the detoxification effect.The coronary arteries supply oxygen-rich blood to the heart muscle as the cardiac veins remove respiratory waste from the blood for optimal function. By impacting BMP A.5, the blood pH is optimized maintaining their alkalinity. It tends to optimize blood cleaning allowing the body to return to the healthy condition. Higher-quality blood delivers the necessary nutrients to the glands for their better function. The left inguinal nerve point is part of BMP A.5 (DURÁN, 2008). The inguinal region refers to the lymph nodes which are essential to the body’s filtration process (ORNELLAS, 2013).
Figure 6: Treatment Protocol – Phase B
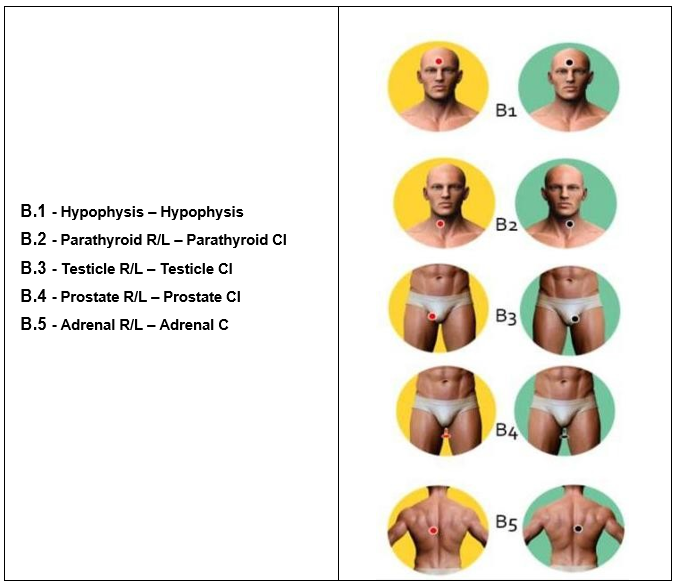
Source: The authors
According to Durán (2014), BMP B.1 is located in the pituitary gland considered one of the most important glands in the central nervous system. It regulates most of the biological processes of the body, considered the center of metabolism. It secretes different hormones as LH stimulating testosterone production in men (the main male hormone), TSH regulating the thyroid function, and FSH stimulating the production of sperm in men. The impact of BMP B.1 with SMF has a modulating action on glandular function. Durán (2008) reports that this dysfunction may cause symptoms such as pituitary adenoma, dysfunction of pituitary hormones, and hypo- or hyperpituitarism. According to Gebara et al. (2002), the gland produces growth hormone (GH), oxytocin, LH, and FSH, as well as TSH, governing the hormonal functions of other glands. Dysfunction in men may cause changes in testosterone production which directly affects the hypogonadism condition.
The reason for impacting the glands is due to the cascade reaction that, when one is dysfunctional, affects the function of the others. This may lead to neuroendocrine and psychosomatic disorders (DURÁN, 2014) which corroborates with the signs and symptoms presented in male hypogonadism.
BMP B.2 balances the parathyroid gland. The alteration of the hormone may alter production to parathyroid hormone (PTH) that causes hypo and hyperparathyroidism also leading to alterations in the thyroid. These alterations cause disorders in calcium and phosphorus metabolism generating hypocalcemia syndrome, decalcification, osteoporosis, osteopenia, and leading to muscular spasms, muscle pain, and male infertility and azoospermia (DURÁN, 2014; BRACCO et al., 2003).
The BMP B.3 modulates testosterone and androgen levels (DURÁN, 2008). According to Bracco et al. (2003), androgens are produced by the testicles and adrenal glands playing an essential role in male sexual and reproductive function. Meanwhile, Gebara et al. (2002) describe that the testicular secretion of testosterone is primarily regulated by the secretion of LH hormone in the pituitary and hypothalamic GH.
The BMP B.4 is related to prostate dysfunction and bladder prolapse, anal and urethral sphincter dysfunction. The treatment of a MB pair may involve other dysfunctions or symptoms that are not related to the site where the magnets were impacted (DURÁN, 2008). According to Goldman (2009), the prostate secretes prostatic fluid that increases sperm motility and, consequently, fertility, as well as sexual potency.
The adrenal gland, related to BMP B.5, connects to the hypothalamus regulating all other glands. Dysfunction of the adrenal gland may be related to chronic fatigue, tiredness, muscle weakness, cortisol dysfunction, and Addison’s disease (DURÁN, 2008). Bonaccorsi (2001) describes that the adrenal gland produces and secretes cortisol providing resistance to stress and helping to manage emotions directly related to the fight or flight response. It also has a modulatory effect on inflammation. It may directly affect ATP production. Sogayar and Figueredo (2003) state that male infertility is rarely associated with a deficiency in the production of gonadotropins but rather caused by the hypersecretion of adrenal steroids which leads to inhibition of the hypothalamic-pituitary axis, preventing normal testicular maturation.Phase C is related to Special Pairs that involve tissue alterations without the presence of microorganisms. In addition to the aspects that lead to hypogonadism symptoms, emotional factors also play a significant role.
Figure 7: Treatment Protocol – Phase C
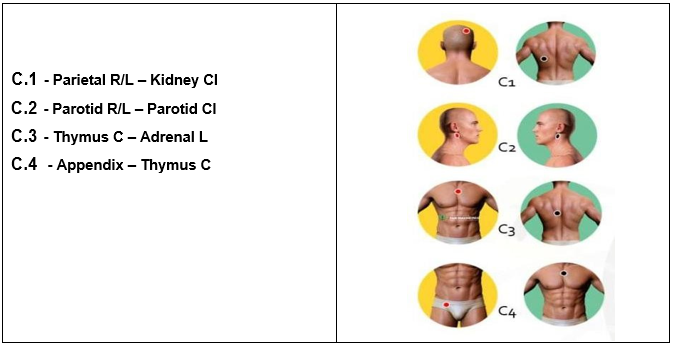
Source: The authors
The treatment with BMP C.1 may assist in the psychosocial aspect. According to Durán (2008), this BMP is located on the lateral part of the skull, however, in his courses, Durán demonstrated the location of the parietal point in the latero-posterior region, as cited in the book “El Codigo Patogeno” (DURÁN, 2010). The BMP is formed with the contralateral kidney point. The parietal point may be replaced by the ear, parotid or parathyroid points, depending on the biological individuality. The point for the formation of the BMP should always be the contralateral kidney point. When the parotid or parathyroid glands are part of the pair, it may indicate hypocalcemia and muscle weakness. It defines organic or psychological manifestations and also for the balance of problems such as depression. This BMP may be applied for a longer time according to the patient’s needs (DURÁN, 2008).
Regarding BMP C.2, Durán (2008) states that dysfunctions in the parotid glands may lead to a decrease in insulin production and secretion, salivary amylase, male sterility, osteopenia, and osteoporosis. Just like the pineal and pituitary glands, the parotid glands have a direct influence on the hormonal production of three other glands, such as the thyroid, parathyroid, and pancreas, modulating the production of insulin, thyroxine, and calcitonin. The hypogonadism condition may generate sterility, weight disorder, osteopenia, osteoporosis, and infertility. The parotid glands secrete saliva, an important element in the digestive process and the protection of the oral mucosa, the site of various pathological processes, both locally and generally (DI HIPÓLITO JUNIOR et al., 1997).
In BMP C.3, the thymus covers immune response, immune suppression and regulation which may lead to diseases such as autoimmunity and immunodeficiency. They may have genetic and/or environmental causes. The adrenal glands secrete aldosterone which is responsible for promoting mineral homeostasis and to produce cortisol (SILVA, 2010). For Durán (2008), the presence of this pair disharmonizes the function of the other glands altering the production of hormones, tissue, and cellular function.
BMP C.4 (Appendix/Thymus C) reflects a condition of dysfunctional deregulation of the immune system altering general hormonal function and the quality of white blood cell and lymphocyte (DURÁN, 2008). The appendix acts on the body’s defenses (JÚNIOR et al., 2007) improving immune competence in the production of lymphocytes and leukocytes, as it stimulates and regulates the immune system (LOPEZ, 2022).
The impact of the BMP described here allows for a general reorganization of the body. The therapeutic system of MB is complex as it involves many concepts from various areas of knowledge; therefore, these processes are still unknown. The organization of the technique in protocols for diseases may allow greater ease of its applicability including the suggestion of the Protocol for the Treatment of Male Hypogonadism.
CONCLUSION
The development of adjuvant treatments in the area of Medicinal Biomagnetism is of great value for the diffusion of the technique. This study is original and important to assist the practice that is constantly expanding. MB protocols may help to close methodological gaps, systematizing their application to be studied with methodological rigor. It is hoped that this protocol may be tested in clinical assays in order to become a complementary tool in the treatment of male hypogonadism.
REFERENCES
BERNARD, Claude. O rim: função, células e biomarcadores. Braz. J. Nephrol. (J. Bras. Nefrol.); 43(1):3-4. 2021
BONACCORSI, Antônio C. Andropausa: Insuficiência Androgênica Parcial do Homem Idoso. Uma Revisão. Arq Bras Endocrinol Metab. V.45. N.2. Pg.123-133. 2001.
BOSSA, Adriane Viapiana. Descrição dos Pares Biomagnéticos. Par Magnético, 4ª Ed. Cascavel, 2019.
BOSSA, Adriane Viapiana. Protocolo de Rastreio do Biomagnetismo Medicinal. Instituto Par Magnético, 1ª Ed. Cascavel, 2021a. Referência do rastreio completo
BOSSA, Adriane Viapiana. Protocolo de Rastreio do Biomagnetismo Medicinal. Cascavel/PR: Editora Independente; Volume 1, Ed. 5, Janeiro – 2021b. Disponível em www.institutoparmagnetico.com.br. Acesso em: fevereiro/2021.
BOSSA, Adriane Viapiana. Biomagnetismo Medicinal Avançado. 2. ed. Cascavel: Instituto Par Magnético, 58 p., 2021c. Referência para os protocolos
BOSSA, Adriane Viapiana. Apostila de Biomagnetismo Medicinal. Cascavel/PR: Editora Independente; Volume 1, Ed. 12. Agosto – 2021d. Disponível em www.institutoparmagnetico.com.br. Acesso em: novembro/2021. Referência para as imagens
BRACCO, Oswaldo Luis; KAYATH, Márcia Jeha; VIEIRA, José Gilberto H. Hormônio da Paratireóide (1-34) no Tratamento da Osteoporose. Arq Bras Endocrinol Metab. V. 47 N.3 junho 2003.
BROERINGMEYER, Richard. Principios de la Terapia Magnetica/Bio-magnetismo. Health Industries, Inc, 1991.
CARDOSO, Ricardo Lopes; NETO, Octávio Ribeiro de Mendonça; RICCIO, Edson Luiz; SAKATA, Marici Cristine Gramacho. Pesquisa Científica em Contabilidade Entre 1990 e 2003. RAE, V. 45 N.2 Pg 34-45, ABR./JUN. 2005.
CALIXTO, Igor Tupinambá. Terapia de reposição da testosterona na DAEM (deficiência androgênica do envelhecimento masculino):uma revisão de literatura: Brazilian Journal of Health Review, Curitiba, v.4, n.1, p.3392-3406 jan./feb. 2021.
CAMPOS, Dário Castro; DIAS, Márcio Carlos Ferreira. A Cultura de Segurança no Trabalho: Um Estudo Exploratório. Revista Eletrônica Sistemas & Gestão. V. 7, N. 4, 2012, pp. 594-604 DOI: 10.7177/sg.2012.v7. n4.a7
CARVALHO, Wanderson Luís de; MAIOLI, Marcos Antonio; MENDES, Luiz Claudio Nogueira; ROZZA, Daniela Bernadete; MINGATTO, Fábio Erminio. Mecanismos da intoxicação do fígado de rato causada pelo gossipol. Pesq. Vet. Bras. 33(3):339-344, março 2013.
DELATTRE, Edson. Ritmos Hormonais Do Pâncreas Endócrino: Dos Fundamentos Cronobiológicos às Implicações Clínicas. Medicina, Ribeirão Preto, N.37: Pg.51-64, jan./jun. 2004.
DELLAZARI, Letícia; FILHO, João Bernardes da Rocha; BORGES, Regina Maria Rabello. Sistema Endócrino e Desreguladores Hormonais: Uma Abordagem CTS Na Formação Inicial De Professores De Ciências. Experiências em Ensino de Ciências – V.5 N.2, Pg. 121-133, 2010.
DI HIPÓLITO JUNIOR, Osvaldo; KREICH, Eliana Maria; HAITER NETO, Francisco; BOSCOLO, Frab Norberto. Sialografia de parótidas clinicamente normais: classificação anatômica e correlação com a função glandular. Rev Odontol Univ São Paulo, v.11, n.2, p.139-145, abr./jun. 1997. https://doi.org/10.1590/S0103-06631997000200011.
FRANK, Bryan L. Biomagnetic Pair Therapy and Typhoid Fever: a pilot study.
Medical Acupuncture, [S.L.], v. 29, n. 5, p. 308-312, out. 2017. Mary Ann Liebert
Inc. http://dx.doi.org/10.1089/acu.2017.1253
GOLDMAN, Suzan Menasce. Ressonância magnética da próstata. Radiol Bras. Mai/Jun; V.42. N.3 Pg.7–9. 2009. https://doi.org/10.1590/S0100-39842009000300002
GONÇALVES, Jessica Batista; CESTARIZYCHAR, Bianca. Utilização De Agrotóxicos, Consumo De Alimentos Com Os Agroquímicos e Seus Efeitos Sobre o Sistema Endócrino. InterfacEHS – Revista de Saúde, Meio ambiente e Sustentabilidade. V. 14 N. 2 – dezembro de 2019.
GEBARA, Otavio C. E; VIEIRA, Núbia W; MEYER, Jayson W; CALICH, Ana Luisa G; TAI, Eun J; PIERRI, Humberto; WAJNGARTEN, Mauricio; ALDRIGHI, José M. Efeitos Cardiovasculares da Testosterona. Arq Bras Cardiol, V. 79 N. 6, 644-9, 2002.
GOIZ DURÁN, Isaac; MARTINEZ, Xabier Zabala; CASTELÁN, Guillermo Mendonza. El Codigo Patogeno. 1. ed. Chapingo, México D. F.: Universidad Autónoma Chapingo, 171 p., 2010.
GOIZ DURÁN, Isaac. El Par Biomagnético. 5. ed. Chapingo, México D. F.: Universidad Autónoma Chapingo, 171 p., 2008.
GOIZ DURÁN, Isaac. El Par Biomagnetico. Editora Universidad De Nuevas Ciências Médicas SC. México 2017.
GOIZ DURÁN, Isaac. Fisiopatologia Bioenergética. Editora Universidad De Nuevas Ciências Médicas SC. México 2014.
JUBIZ, Willina; CRUZ, Eduardo A; Hipogonadismo masculino: Causas, genética, diagnóstico y tratamento. Editora Médica del Valle. Colomb Med; 84-91 Vol. 38 Nº 1, 2007 (Enero-Marzo) 2007.
JUNIOR, Flavio; LAVRATTI, Vinicius B.; ROTA, Cristiane de B.; FARNEDA, Lais P.; FRONZA, Dilson. Correlação da Avaliação Clínica e Laboratorial no Rastreio do Hipogonadismo Masculino. FAG Journal of Health (FJH), v. 3, n. 2, p. 140-146, 27 jun. 2021.
JÚNIOR, Marcelo Eustáquio Montandon; MONTANDON, Cristiano; FIORI, Gustavo Ribeiro; FILHO, Carlos Alberto Ximenes; CRUZ, Fernanda Coelho Barbosa da. Apendicite Aguda: Achados na Tomografia Computadorizada – Ensaio Iconográfico. Radiol Bras; V.40. N.3. Pg.193–199. 2007.
LOPES, Ana Lucia Mendes; FRACOLLI, Lislaine Aparecida. Revisão Sistemática de Literatura e Metassíntese Qualitativa: Considerações Sobre Sua Aplicação na Pesquisa em Enfermagem. Texto Contexto Enferm, V.17(4) Pg. 771-8. Florianópolis, Out-Dez. 2008.
LOPEZ, Mônica G. C; “Subsistema conyugal y andropausia en pacientes del primer de atención de salud”. Requisito Previo Para Obtar Por El Título De Especialista En Medicina Familiar Y Comunitaria. Universidad Técnica de Ambato Facultad de Ciencias de la salud posgrado programa de especialización en medicina familiar y comunitaria tercera cohorte modalidad de titulación proyecto de investigación. Ambato – Equador, (marzo 2022).
MAGALHÃES, Ana M. M.; CUNHA, Debora R. M. F.; MOURA, Gisela M. S. S.; URBANETTO, Janete S.; WEGNER, Wilian; OLIVEIRA, João Lucas C. Ambiente da prática profissional da equipe de enfermagem em unidades de internação de hospital universitário. Rev Gaúcha Enferm. V. 41. N.01-08. Pg. 2020: e 20190460. doi: https://doi.org/10.1590/1983-1447.2020.20190460.
MARTÍNEZ, David Goiz. Guía de Pares Biomagnéticos primer nivel. Ciudad de México: Biomagnetism Research Institute, 142 p., 2017a.
MARTÍNEZ, David Goiz. Guía de Pares Biomagnéticos segundo nivel. Ciudad de México: Biomagnetism Research Institute, 120 p., 2017b.
MARTÍNEZ, David Goiz. Manual del Biomagnetista. Ciudad de México: Biomagnetism Research Institute, 177p., 2018.
MASA, Justus; BARWE, Stefan; ANDRONESCU, Corina; SCHUHMANN, Wolfgang. On the Theory of Electrolytic Dissociation, the Greenhouse Effect, and Activation Energy in (Electro)Catalysis: A Tribute to Svante Augustus Arrhenius. Chemistry. V. 25, N. 1, p. 158-166, 2019. https://doi.org/10.1002/chem.201805264
MARINHO, Antônio Ferreira. Amígdalas e Adenoide – da Infecção à Obstrução. Revista Portuguesa de Otorrinolaringologia e Cirurgia Cervico-Facial. V.48 N.1. março de 2010.
MARTITS, Anna Maria; COSTA, Elaine Maria Frade. Hipogonadismo masculino tardio ou andropausa. Revista da Associação Médica Brasileira [online]. 2004, v. 50, n. 4 [Acessado 19 outubro 2022], pp. 358-359. Disponível em: <https://doi.org/10.1590/S0104-42302004000400018>. Epub 14 Jan 2005. ISSN 1806-9282. https://doi.org/10.1590/S0104-42302004000400018.
MATOS, Amélio F. Godoy; MOREIRA, Rodrigo O.; GUEDES, Erika P. Aspectos Neuroendócrinos da Síndrome Metabólica: Arq Bras Endocrinol Metab vol 47 nº 4 agosto 2003.
MELO Márcio C. DE; SOARES, Amanda N.; BARAGATTI, Daniela Y. Hipogonadismo masculino ou andropausa: Estudo de revisão integrativa da literatura: Rev enferm UFPE [on line]. Recife, V.7(esp). Pg.898-909, mar., 2013.
MOLLE, Ana Carolina M.; MATHEUS, Ivna C. N.; LUCENA, Jeane R.; NUNES, Lianna; OLIVEIRA, Lívia S.; SHOLL-FRANCO, Alfred. Fatores psicofisiológicos na terapia de reposição hormonal em homens. Ciências & Cognição; V. 3. Pg. 4-9. 2004.
ORNELLAS, Antônio Augusto. Linfadenectomia inguinal e pélvica. Urologia Brasil, 1234-55. 2013.
PAIM, Jairnilson S. Atenção à saúde no Brasil. In: BRASIL. Ministério da Saúde. Saúde no Brasil: contribuição para a agenda de prioridades de pesquisa. Brasília: Ministério da Saúde, Pg.14-40. 2004.
PEREIRA, Renata J. e CARDOSO, Maria G. Metabólitos secundários vegetais e benefícios antioxidantes. J. Biotec. Biodivers. V. 3, N.4: Pg. 146-152, Nov. 2012.
PARRA, Isabelle Ascanio. “Estudio Comparado De La Aplicación De Diferentes Técnicas – Acupuntura y Biomagnetismo – En El Tratamiento Efectivo De La Obesidad” Tesina (Fin de Curso de Acupuntura, CEMETC). Centro de Enseñanza de la Medicina Tradicional ChinaEscuela Dragón de Jade – Carrera de Medicina Tradicional China Caracas. Marzo de 2020.
ROHDEN, Fabiola. O homem é mesmo a sua testosterona: promoção da andropausa e representações sobre sexualidade e envelhecimento no cenário brasileiro: Horizontes Antropológicos, Porto Alegre, ano 17, n. 35, p. 161-196, jan./jun. 2011.
SILVA, Bernardo Melgaço da. A Glândula Timo e as Técnicas de Cura da Medicinal Holística Tradicional. Revista de Psicologia. Ano 4, N. 12, novembro – ISSN 1981-1179. 2010.
SILVA, Juliana Barbosa. Papel da nutrição no processo de destoxificação. Braz. J. of Develop., Curitiba, V. 6, N 7. Pg.42416-42425, jul. 2020.
SOGAYAR, Ana. M. C. B.; FIGUEREDO, Luiz F. P. de. Infertilidade Masculina associada à deficiência da 21 hidroxilase. Rev Assoc Med Bras; 49(1): 1-23. 2003.
TANO, Simone Sayome e SILVÉRIO-LOPES, Sandra. Magnetoterapia e Magnetopuntura. Silvério-Lopes Ed. Pg. 50-60. 2013. DOI: 10.7436/2013 anac. 04. ISBN 978-85-64619-12-8.
WERNECK, Marcos Azeredo Furquim; FARIA, Horácio Pereira; CAMPOS, Kátia Ferreira Costa; Protocolos de Cuidado à Saúde e de Organização do Serviço. Núcleo de Educação em Saúde Coletiva da Faculdade de Medicina/UFMG; Belo Horizonte Nescon UFMG Editora Coopmed (Nescon)). 90pg. 2009.
1Student of the Graduate Program in Biomagnetism and Bioenergetics Applied to Health, Faculty of Technology – FATEC, Curitiba – Paraná – Brazil.
2Co-supervisor of the Graduate Program in Biomagnetism and Bioenergetics Applied to Health, Faculty of Technology – FATEC, Curitiba – Paraná – Brazil.
3Supervisor of the Graduate Program in Biomagnetism and Bioenergetics Applied to Health, Faculty of Technology – FATEC, Curitiba – Paraná – Brazil.