REGISTRO DOI: 10.5281/zenodo.7905204
Aurélio D. Santos1, Antônia de O. Silva2, Karine V. Tako3, Lara B. Bottcher4, Auricélia D. Santos 5, Marcia A. B. C. Pereira6, Ronaide P. Santos6, Ana G. G. Pereira7, Shirley k. C. de Matos8
ABSTRACT
Background: In Brazil, the family is responsible to provide care for the elderly. Although it is compulsory for the sons to support their parents in old age, according to Brazilian legislation, older adults constitute a social category that includes a high percentage of extremely frail people. Objective: To investigate, through a systematic review, mistreatment of the elderly in long-term care institutions. Design: The study was carried out using the systematic review method with qualitative meta-synthesis. Methods: For this, the acronym of pico was characterized, and the research carried out in the databases PubMed, portal VHL, Plataforma Capes, Pedro and Cochrane. In the search, the terms / descriptors in Health Sciences were used in English. Language: Aged, Homes for the aged and Elder Abuse and their representatives in Portuguese: Idosos, instituições de longa permanência para idosos and abusos contra idosos. Results: 628 articles were found (365 PubMed, 6 Cochrane, 103 Capes, 143 VHL, 11 Pedro), and five were included. The data distribution and density estimation calculations were performed. The most homogeneous treatments were physical, psychological, sexual, negligence and verbal. Conclusion: The institutionalized elderly may suffer mistreatment by caregivers and by their peers living in long-term care facilities.
Keywords: Elderly, Long-term Care Institution , ill-treatment.
1 INTRODUCTION
The aging of the population is a worldwide phenomenon. According to the World Health Organization (WHO)(1) in 2025, there will be 1.2 billion people over the age of 60, and people aged 80 and over being the fastest growing segment of the population. In Brazil, projections estimate that there will be 58.4 million elderly people (26.7% of the total), in 2060 [2].
According to the WHO, mistreatment of the elderly can be defined as: single or repeated mistreatment or even omission, causing suffering or distress and occurring within a context of trust; that is, it can occurs inside or outside home environment by a family member or by persons in a power relation over the elderly person. Common forms of violence against older adults includes but are not restriceted to physical abuse, psychological abuse, sexual abuse, abandonment, financial abuse, neglect and self-neglect [3,4].
The difficulty of identifying violence against the elderly is notorious, since it is not only physical, but also causes social, psychological and moral damages. Regardless of the type of abuse, it will result in unnecessary suffering, injury or pain, loss or violation of human rights and decline of quality of life [5].
Long-term or long stay care institutions (LTCI) for the elderly are responsible for satisfying the needs of the elderly in terms of housing, food, health and social cohabitation through work social services, medicine, psychology, nursing, physical therapy, occupational therapy, dentistry, nutrition and other services [6].
There is a well known concern about the damage that institutionalization can bring to the elderly, such as segregation, difficulty in providing equal and simultaneous treatment for all residents and a state of control. Thus, public policies have been developed in the sense to encourage the permanence of these individuals with their family [7]. However, in many cases, being with the family does not necessarily mean protection, since neglect and physical, psychological, emotional and moral mistreatment to the elderly is not a new fact [8].
Considering this, as well as the importance of producing new reflections that help to fight against elder abuse in different dimensions, the following guiding question was delimited for this study: Does the mistreatment occur in elderly people residing in LTCI? Facing this inquiry, we aim to investigate what kind of mistreatment occurs and who is the aggressor of elderly people residing in such institutions.
However, this work is justified based on the need to verify the violence suffered by the older adults, due to the loss of youth and their increased vulnerability and frailty in the course of life; since violence against the elderly is present in all social strata, not only in the lower classes, and even in the health services themselves. Thus, understanding the context in which violence against institutionalized people occurs empowers health professionals, making it possible to diagnose the type of mistreatment and the aggressor. In addition, it also helps to assist the elderly person in a preventive way.
This work is extremely important for professionals, especially in the health care area, who face abuse in institutionalized elderly people more frequently than other professionals. It is also of great importance to stimulate the State in order to be more attentive to this segment of population, which is experiencing a great demographic change, requiring more care, especially in LTCI.
2 METHODS
It is a systematic review with meta-synthesis, which is characterized by problem solving from identification, labeling, in order to test the relationship between these variables [9].
The objective of the systematic review is to seek consensus on some specific topics and to synthesize the knowledge of a given area through the formulation of a question, identification, selection and critical evaluation of scientific studies contained in electronic databases. From this process, it allows, in addition to deepening the knowledge about the researched subject, to point out gaps that need to be fulfilled through new investigations [10, 11].
The systematic review with meta-synthesis, which is characterized in a qualitative way, is defined as interpretative integration of qualitative findings, that is, interpretative data synthesis [12]. Qualitative meta-synthesis presents a new interpretation of the results, since it can not be found in any primary research report, and since they are inferences descendent from the fact that all the articles have become a sample in their entirety. This type of research aims at strengthening the role of qualitative studies in health sciences research, improving the application of research results in clinical practice and thus exploring a body of qualitative knowledge to support theory, practice, research, and health policies [11, 13].
According to the recommendations of the Main Items to report systematic reviews and meta-analyzes (PRISMA), which is a checklist of 27 items, researchers are recommended to use at least the items with the highest methodological qualification that can not be missing in an analysis of systematic review. These main items are suggested by PRISMA in a standardized summary table, which we used in our research, and a flowchart to guide researchers to improve systematic review reports [14]. This procedure was used to delineate the screening of articles, aiming at filtering the best scientific evidence, mainly characterizing the studies that present better methodological rigor.
The research was developed based on the construction of a PICO acronym, where it was formulated the adequate construction of a research question, in order to facilitate the search in databases and to avoid unnecessary search. PICO represents an acronym for P – Patients, I – Intervention, C – Comparison or control and O – outcomes, which means clinical outcome or outcome. In our study, we considered: P = elderly, I = mistreatment of the elderly, C = mistreatment and long-term care institutions for the elderly, O = is there any abuse in long-term care institutions for the elderly?
The search was carried out in databases such as PubMed, in the BVS portal (searched in all available databases), Plataforma Capes, Pedro and Cochrane. In the search, the following terms / descriptors in Health Sciences were used in the English language: Aged, Homes for the aged and Elder Abuse and their representatives in Portuguese: Idoso, Instituição de Longa permanência para idosos and maus-tratos contra idosos. Tracing the publications, the Boolean operators “AND” and “OR” were used in order to combine the terms / descriptors mentioned above.
In the collection of articles, the following inclusion criteria were considered: complete articles free of charge and fully available, target population composed of institutionalized elderly people of both sexes, aged 60 years and over, studies on mistreatment of institutionalized elderly people, publications in English, Spanish, Portuguese and without limitation of the publication year. Exclusion criteria was: systematic review, literature review, theses and annals of congress.
The selection of the studies was carried out between April and May 2017 by two independent evaluators. This procedure occurred in the following steps: in the first step, the search was performed combining descriptors and Boolean operators ( Aged and Homes for the Aged and Elder Abuse) in the PubMed – which resulted in 365 articles, BVS – 143 articles, Cochrane – 6 articles, Pedro – 11 articles, Plataforma Capes – 103 articles, totalizing 628 articles.
In the second stage, the articles were filtered with the inclusion criteria specified in the databases; which resulted in PubMed – 28 articles, BVS – 78 articles, Cochrane – 6 articles, Pedro – 11 articles and Plataforma Capes – 30 articles, being selected for a total of 153 articles. 475 articles were excluded, being 133 articles because they were not carried out in LTCI, 46 articles because the sample had both adults and elderly people, 147 articles were not related to mistreatment and 149 articles because they were not available in the free full version.
In the third step, the titles and abstracts of the articles were critically read, and resulted in PubMed – 15 articles, BVS – 10 articles, Cochrane – 01 articles, Pedro – no articles and Plataforma Capes – 10 articles, 36 articles were then selected. A total of 117 articles were excluded, 26 articles were related to social / psychological support, 8 duplicate articles, 11 articles related to the definition / contextualization of mistreatment, 23 articles did not specify the type of mistreatment, 37 articles did not specify the type of aggressor and 12 articles were not available for reading.
In the fourth stage, the prism table was used as criterion of methodological qualification for final inclusion of the articles, being analyzed the following aspects: a) authors and year; b) sample; c) study design; d) scientific journal; e) category of study; f) main findings; g) limitation of the study; and h) conclusion. However, after a complete reading of these qualifying criteria, only 05 articles were selected. In this final phase, 31 articles were excluded: 04 articles did not explain how the authors delimited the sample, 03 articles presented inconsistency in the study design, 08 articles did not present mistreatment and aggressor, 07 articles presented problems in the main findings (the authors generalized the results only reported that the elderly were mistreated and / or the aggressor was not identified in the surveys carried out by coordinators of LTCI and 9 articles did not present the limitations of the study.
The statistical analysis of the meta-synthesis was performed through calculations of data distribution and density estimation using the program Stata 14.0 and Shannon-Wiener Index using the BioEstat 5.0 program.
3 RESULTS
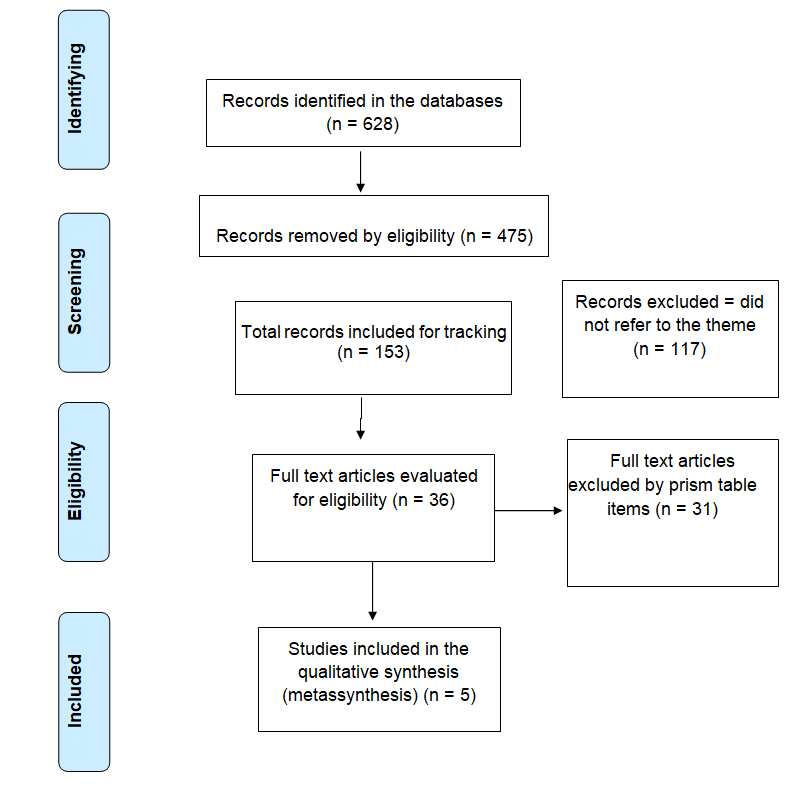
In the general search of the articles were found 628 articles (365 PubMed, 6 Cochrane, 103 Plataforma Capes, 143 BVS, 11 Pedro). After filtering by two independent evaluators, through the eligibility criteria; and also by the methodological parameters according to the Prism table, 5 articles were selected for the systematic review. Figure 1 presents the synthesis of the article selection process.
Figure 1 (PRISMA2009FlowDiagram): Identification and selection flowchart for articles for systematic review on elder abuse that remain in long-term institutions for the elderly.
In this systematic review five articles that met the methodological criteria established by the Prism Table were analyzed. In order to facilitate the analysis and presentation of the results, the description of the findings is presented, according to the Prism Table for each selected article.
Table1. Data from selected articles in the systematic review of elder abuse in Long Stay Care Facilities for the Elderly
Graph 1 and Table 2 below show the quantitative synthesis (Table 1) of the qualitative information (Chart 1) extracted from the studies.
Graph 1: Shannon-Wiener diversity index for mistreatment of elderly people in Long-Term Care Institutions for the Elderly.
Table 2: Qualitative information extracted from the studies.
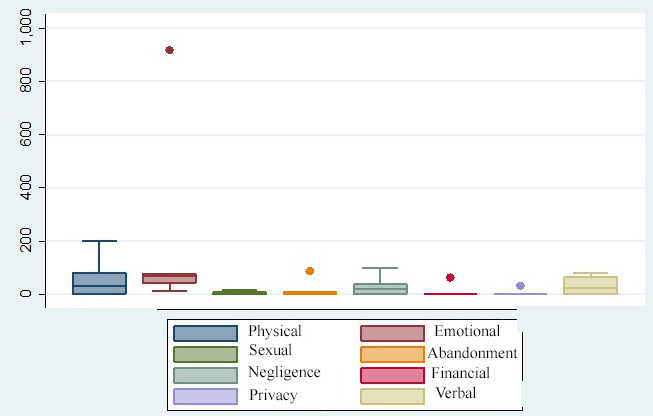
The frequency of citations and samples for each abuse against the elderly in long-term institutions is shown on the graph in the sequence.
Graph 2: Distribution of samples of elder abuse in Long-term Institutions for the Elderly.
The density estimation was analyzed for the four most frequent abuses (Graph 3, 4, 5 and 6).
Graph 3: Density estimation for Physical-type mistreatment of elderly people in Long-Term Institutions for the elderly.
Graph 4: Density estimation for Emotional mistreatment of elderly people in Long-stay Institutions for the elderly.
Graph 5: Density estimation for mistreatment type of neglect of elderly people in institutions for long stay for the elderly.
Analyzing the estimation of Kernel density – density for mistreatment, it was possible to observe a variation of 19% to 39%, this finding is quite significant in the context of violence with the elderly person; because it reveals a considerable percentage of mistreatment that usually occurs in LTCI for the elderly.
Graph 6: Density estimation for verbal mistreatment of elderly people in Long-Term Institutions for the elderly.
Regarding the type of aggressor, it was not possible to perform the meta-synthesis because of the heterogeneity of the studies. Thus, the findings were presented in Table 3 to better explain the results we found in this systematic review.
Table 3.Reports of the main aggressors of the elderly living in long-stay institutions for the elderly.
4 DISCUSSION
Type of mistreatment:
When we analyzed the distributions of samples referring to types of mistreatment, it was evidenced in the studies that the most frequent categories were physical abuse and neglect among the investigated studies.
In a survey about the perceptions of abuse related to care in LTCI for the elderly in Uruguay, the authors verified that the elderly suffered mistreatment from their caregivers; and the abuse included verbal, physical, sexual abuse, neglect, robbery, physical neglect (family and social neglect, denial of food and water) and psychological neglect (isolating the elderly person in the nursing home). The authors also reported that these types of mistreatment occurred more independent elderly people, explaining that mistreatment occurs due to the lack of organization and planning of LTCI for the elderly, associated with the precarious training of caregivers and discrimination of the institutionalized elderly person [15].
In relation to the aforementioned study, it was perceived that verbal abuse could be recognized in the form of yelling (the caregiver shouts, answers rudely or orders them to shut up), insensitive treatment (caregivers did not consider elderly’s needs to chat and did not have patience and time to interact with them during daily activities), the venting (when the elderly person missed relatives and wanted to talk about it, but the caregiver pretended to listen and changed the subject ignoring the situation) and derogatory comments (the caregiver commented that the elderly did not know how to do anything else alone, mentioned in front of others [elderly people or visitors] who could not see or hear well, did not know how to walk, was lazy or in bad mood).
However, physical abuse can be recognized in LTCI for the elderly, when caregivers hit them against the wall when performing activities of daily living, squeezing / tightening upper and / or lower limbs when changes position, physical coercion (forcing, intimidating or threatening the elderly person to carry out any activity or situation), undressing the person by pulling their clothes with violence, causing injuries and / or bruising, since the elderly’s skin is frequently frailer and dehydrated, susceptible of such types of trauma.
A study verified the aggression of the elderly versus elderly (resident-resident) living in LTCIAuthor’s findings included primarily verbal assaults (personal integrity and bedroom problems resulting in 56 events)/ aggressive reactions (hostile interpersonal interactions) resulted in 38 events; inappropriate sexual behavior in which a younger elderly person performed against an older person resulted in 7 events ; and moments / situations that there were no motives for mistreatment among the elderly, but there were reactions of misunderstanding by only one part resulted in 21 events. The authors reported that the great variety of situations of resident-resident mistreatment may be due to the structural inadequacy characteristics of LTCI for the elderly. However, the authors suggested that such a problem can be solved with adaptations in the structure of these institutions for older people [16].
Pillemer et al. (2012) found interesting results and not well investigated in the scientific literature, especially in Brazil, where up to the present moment no complete, free and eligible article among the criteria approached in our study has been identified about this theme. We can observe that mistreatment among residents may be related to the higher number of elderly people living in these institutions, leading to agglomerations in rooms, corridors, dining rooms, visiting rooms and other facilities. This can lead to greater probability of discussion / aggression among the elderly, due to the loss of their personal, environmental and social intimacy. It is important to consider that the closer contact of discontented residents can incite possible aggressions during in simple situations, such as listen to music louder in the room, ask several times to go to the bathroom, ask for water, ask to turn off the television, turn off the light in the room, bump into the corridors and others. Situations of this type when performed by a dependent elderly person, who keeps repeating the same speech of help, and the caregiver that is currently busy, can trigger misunderstandings with possible verbal and / or physical aggression [16].
A study conducted a survey through reports from family members about abuse in LTCI for seniors in Michigan. The authors reported that older people may also be abused by employees (caregivers or visitors) in their homes, as well as experience abuse from other residents. The forms of mistreatment were physical, verbal and sexual abuse. Authors also reported that it was possible that family members who reported personal abuse, had a general negative view of nursing homes where their relatives were receiving care. In their view, the abuse among residents should have occurred in that environment as well. However, no empirical study has found that dissatisfied family members tended to make random accusations against other residents and visitors in nursing homes. On the other hand, it was possible that family members who reported abuse of staff were more vigilant against all types of abuse compared to other family members who did not report personal abuse [17].
We observed that it was used a different type of interview approach through reports with perspective of relatives as an investigative focus of elder abuse.This type of investigative evaluation focused on family knowledge is a very interesting approach, because for this type evaluation it is necessary that the family has contact with the elderly person in LTCI; especially in the moments of visitation, so that the elderly can report situations of mistreatment to their family. Even though this approach about the most common types of mistreatment evidenced by the authors were reported by elderly’s family members, such findings are in line with the findings of Borda and Yarnoz (2015) and Pillemer et al. (2012) because are related to physical abuse (verbal interpersonal interactions, personal integrity and bedroom problems) and inappropriate sexual behavior. In the same perspective of the type of aggressor, similar reports occurred only in the study of Borda and Yarnoz (2015) – the caregiver. According to Pillemer et al. (2012), to which the perspective of investigation was different from elderly to elderly (resident-resident), the type of aggressor was already a target to be investigated [13, 15, 16].
In the survey of physical abuse evaluation of older people in LTCI from the perspective of the family, an investigation of the incidence of physical abuse classified the type of physical abuse and which of these would be the most reported by relatives. It was reported that 110 (24.3%) of the elderly residents of the sample (n = 452) were subjected to physical abuse by the caregiver (nursing team). However, the types of physical abuse most commonly found in LTCI were physical mistreatment (knocking, pushing, kicking), n = 44 (27%); Mistreatment with the inappropriate use of restrictions (from taking to the toilet, not taking to shower, forced feeding), n = 103 (62%); Sexual abuse by the caregiver, n = 18 (11%) [17].
However, Zhang et al. (2012) and Schiamberg et al. (2012), using a similar investigative approach, where the relatives were interviewed, found very similar results both in the type of aggressor and in the definition of the type of mistreatment. This similarity of results may, to a certain extent, elucidate that the main aggressor is the caregiver and that the forms of elder abuse carried out against the elderly in LTCI, for the most part, are physical, verbal and sexual. It should be noted that the relative frequency of sexual abuse by the caregiver is always a smaller percentage when compared to the other abuses mentioned [17, 18].
In the reports of family members about abuse in LTCI for the elderly in Michigan, their findings have revealed the following types of mistreatment: physical mistreatment – 31; treatment of ill-treatment – 89; verbal mistreatment – 67; emotional or psychological mistreatment – 78; negligence – 99; sexual misconduct – 10 and material exploitation – 64. Thus, the problem of elder abuse in LTCI may increase as a large number of elderly individuals need home-based care and are abandoned in such institutions [19].
These findings also clearly show the same types of mistreatment found in the aforementioned studies. Only in a different way is it possible to characterize the fact that 89 elderly people needed treatment due to mistreatment, thus classifying physical violence against the elderly. Having another important finding, but not repeated in other studies frequently, emotional mistreatment, in a very significant amount of 78 elderly [19].
Type of aggressors:
According to Table 3, it was observed in the selected studies that the main abusers (neglect) against the institutionalized elderly were the caregivers and the residents themselves.
13 forms of aggression were among residents themselves, LTCIs managers pointed out that mistreatments were practiced by doctors, caregivers and the residents themselves. Relatives reported abuses by the employees, visitors and the elderly themselves, and an author described physical abuse by nursing professionals, while other studies argue that the family described that abuse and neglect came from visitors as well as caregivers [15, 16, 17, 19].
Abuse involves not only the elderly penalized for mistreatment, but also their family members and the community. In the social sphere, there should be an expressive participation of health care professionals to assist the victim, in an articulated and interdisciplinary way with other social sectors, in order to protect the elderly and punish those responsible.
In this study, the main limitation was observed in the large number of excluded articles, especially because they were not fully available. In addition, other excluded articles were related to elder abuse in the community or related to reflective studies about the characterization of types of mistreatment and its association with the impact on the quality of life of the elderly. Finally, another important limitation is the fact that we did not find any Brazilian studies that presented methodological rigor on the subject. This characterizes the lack of national data on this subject, making it difficult for us to detect such mistreatment at the local level, consequently affecting specific actions to prevent elderly abuse, to guide family members, caregivers, directors of the institutions, and to provide support to the very victim who is the elderly person.
5 CONCLUSION
It was observed that the types of mistreatment most commonly suffered by the elderly were physical, psychological, sexual, verbal, and negligence. However, residents and caregivers are the main offenders.Elderly abuse is an important public health problem with visibility in the contemporary world, the scientific knowledge produced on the subject, especially in Brazil, is still scarce.
It is necessary to do other research on this subject, due to the large increase of LTCIs on a worldwide level and the assumption that the process of institutionalization of the elderly is something that grows every day, such elderly people need to live in this type of housing with dignity and quality of life.
REFERENCES
1: World Health Organization, IPEA. Missing Voices: views of older people on elder abuse. Geneva: World Health Organization: 24, 2002.
2: Instituto Brasileiro De Geografia E Estatística (IBGE). Censo demográfico: sinopse dos resultados do Censo 2013. Rio de Janeiro.[cited 2011 fev. 25], 2013. http://www.censo2013.ibge.gov.br/sinopse/webservice/
3: Pavlik VN, Hyman DJ, Festa NA.Quantifying The Problem Of abuse and neglect in adults-analysis of a statewide database. Journal Of The American GeriatricsSociety. 49(1), Malden – USA, 2001.
4: Minayo MCS Violência: um problema para a saúde dos brasileiros. In: BRASIL, Ministério da Saúde. Secretaria de Vigilância em Saúde. Impacto da violência na saúde dos brasileiros.Ministério da Saúde: 9-41, Brasília, 2005.
5: Leite MT, Hildebrandt LM, Santos AM. Maus-tratos a idosos no domicílio: concepção de familiares. Revista Brasileira de Geriatria e Gerontologia. 11(2): 209-221, Rio de Janeiro, 2008 [cited 2018 apr 16]. Available from: http://www.redalyc.org/pdf/4038/403838778007.pdf
6: Sociedade Brasileira De Geriatria e Gerontologia (SBGG). Instituição de longa permanência para idosos: manual de funcionamento/ Institution Of Long Permanence for aged. São Paulo, 2004.
7: Tomasini SLV, Alves S. Envelhecimento bem-sucedido e o ambiente das instituições de longa permanência. RBCEH. 4(1): 88-102, Passo Fundo, 2007.
8: Porto I,Koller SH. Violência contra idosos institucionalizados. Revista de Psicologia do Vetor Editor. 9(1): 1-9, Rio grande do sul, 2008.
9: Thomas JR, Nelson JK, Silverman SJ. Métodos de Pesquisa em Atividade Física. 5ed. Porto Alegre: Artmed.2007.
10: Munoz SIS, Takayanagui AMM, Santos CB, et al.O.Revisão sistemática de literatura e metanálise: noções básicas sobre seu desenho, interpretação e aplicação na área da saúde. In: Anais do 8º Simpósio Brasileiro de Comunicação em Enfermagem. Universidade de São Paulo,Ribeirão Preto, 2002.
11: Lopes ALM,Fracolli LA. Revisão sistemática de literatura e metassíntese qualitativa: considerações sobre sua aplicação na pesquisa em enfermagem. Texto & Contexto- Enfermagem. 17(4): 771-178, São Paulo, 2008 [cited 2018 apr 16]. Available from: http://www.producao.usp.br/bitstream/handle/BDPI/3771/art_LOPES_Revisao_sistematica_de_literatura_e_metassintese_qualitativa_2008.pdf?sequence=1&isAllowed=y
12: Matheus MCC. Metassíntese qualitativa: desenvolvimento e contribuições para a prática baseada em evidências. Acta Paul Enferm. 22(-): 543-545, São Paulo, 2009.
13: Sandelowski M, Docherty S, Emden C. Focus on qualitative methods qualitative metasynthesis: issues and techniques. Res Nurs Health. 20(4): 365-371, 1997.
14: Moher D, Liberati A, Tetzlaff J, et al. Principais itens para relatar Revisões sistemáticas e Meta-análises: A recomendação PRISMA. Epidemiol. Serv. Saúde. 24(2), Brasília, 2015.
15: Borda N, YarnozA.perceptionsof abuse in nursing home care relationships in uruguay. Journal of transcultural nursing. 26: 164-170.Uruguay, 2015.
16: Pillemer K, Chen EK, Kimberly S, et al. Resident-to-resident aggression in nursing homes: results from a qualitative event reconstruction study.TheGerontologist. 52(1): 24-33, 2011 [cited 2018 apr 16]. Available from: http://europepmc.org/backend/ptpmcrender.fcgi?accid=PMC3265555&blobtype=pdf
17: Schiamberg LB, Oehmke J, Zhang Z. et al. Physical abuse of older adults in nursing homes: a random sample survey of adults with an elderly family member in a nursing home.Journal Of Elder Abuse andNeglect. 24(19): 65-83, 2012.
18: Zhang Z, Page C, Conner T, et al. Family Members’ Reports of Non-Staff Abuse in Michigan Nursing Homes. Journal of Elder Abuse and Negligência. 24(-): 357-369, 2012.
19: GRIFFORE JR, BARBOZA GE, MASTIN T, et al. Family Members’ Reports of Abuse in Michigan Nursing Homes.Journal of Elder Abuse & Neglect. 21(-): 105-114, Michigan, 2009.
TABLES, GRAPHS AND FIGURES.
Table 1.Data from selected articles in the systematic review of elder abuse in Long Stay Care Facilities for the Elderly– PRISMA
Authors / yearSample Design of study Journal Category Main Findings Limitation Conclusion Pillemer et al. (2012) Analysis of 122 reconstructions of events Social-ecological model The Gerontologist Exploratory study
The analysis of the 122 reconstructions of events identified 13 main forms of ARR, grouped into five themes. The resulting picture demonstrated the heterogeneity of RRA types, the importance of considering personal, environmental and trigger factors, potential emotional and physical damage to residents.Category 1 – invasion of privacy or personal integrity: Incursion in personal space (7); Invasion of privacy of the room (16); Eliminating a path through congestion (8); Inappropriate assistance (2); Room Problems in Category: Misunderstandings of Roommates (12); Belligerent roommate (11); Category 3. Hostile interpersonal interactions: irritated attempts at social control (13); Arguments (7); Disproportionate response to normal interaction (7); Fondling or playing (6); Accusations (5); Category 4 – unprovoked actions: unprovoked actions (21); Category 5 – inappropriate sexual behavior: inappropriate sexual behavior (7).The study has three limitations that point to future research needs. First, the number of facilities was small. Second, the study was limited to the New York region. There are no clear reasons for the hypothesis that the types of RRA encountered would vary between facilities (although the occurrence frequency would likely vary) or by region. However, to ensure the generalization and transferability of the findings, it would be ideal to include a larger number of facilities representing metropolitan and non-metropolitan areas in future studies. Finally, the methodology used does not allow inferences at the resident level.
The central finding of the study is that ARR covers a wide range of behaviors, rather than being a discrete phenomenon. The environmental characteristics of a nursing home are likely to contribute to ARR. Some of the types of events we detail in this article seem appropriate for environmental modifications.This article focused on analyzing and categorizing events; As such, our goals were primarily descriptive. Based on this effort, an important task for researchers is to begin to identify RRA-specific risk factors. These results suggest the need for person-centered environmental interventions to reduce ARR, as well as for new research on the subject.
Griffore et al. (2009)
452 respondents
Cross-sectional study with several retrospective sequences
Journal of elder abuse & neglect Qualitative Study
The majority of the residents in this analysis were women (73.2%), Caucasian (91.4%) and widows (64.8%). Respondents were asked if the person in the nursing home had experienced various types of abuse and neglect by staff or other caregivers in the past 12 months. The number of valid respondents was as follows: physical mistreatment 31; Ill-treatment 89; Verbal mistreatment 67; Emotional or psychological mistreatment 78; Negligence 99; Sexual misconduct 10 and material exploitation 64.
Respondents may be wrong in their assessments of what they know about abuse and neglect in nursing homes, and it is very difficult to measure the accuracy and reliability of their knowledge. In addition, it is not clear that any measure of proximity will actually prove how much the respondents know about abuse and neglect.
The problem of elder abuse in long-term care facilities may increase as a large number of elderly individuals need home-based care. Thus, the importance of having sensitive and accurate measures of actual incidents of nursing home abuse will increase in the future.
Borda eYarnoz, (2015)
23 participants who were deliberately and theoretically chosen
wereinterviewed
A qualitative study with ethnographic analysis.
Journal Of Transcultural NursingQualitative Study
The types of elder abuse practices detected by caregivers were physical neglect, such as family and social neglect, denial of food and water, and psychological neglect in the form of isolation in the nursing home itself. Verbal abuse consisted of shouting, insensitive treatment, and derogatory comments for dependent individuals. Physical abuse included shocks to the wall, squeezing the upper limbs, physical coercion, stripping the person of pulling their clothes, sexual abuse and robbery.
The present study has limitations due to the impossibility of including nursing homes with a higher socioeconomic level. Separately, the lack of authorization to make participant observations at all centers, represented a limitation in terms of learning about the culture of the elderly home in depth.
A cultural context of discrimination against the elderly and other factors converge to perpetuate the abuse and suffering of the elderly in nursing homes: lack of adequate regulations covering safety and quality of care, lack of a care model and inspections lack of minimum training requirements for caregivers and lack of support in situations where there is a need for psychic and spiritual repercussions.
Zhang et al.(2012)In this study, the analytical sample was restricted to the 964 knowledgeable family members of, or adults responsible for, a nursing home resident. The sample comes from two waves of the Michigan Household Survey with family members in nursing homes conducted in 2005 and 2007.
This is the first generalizable randomized sample of non-personal abuse in nursing homes from the perspective of family members. It is also one of the first studies that did not rely on nursing homes to report incidents or restrict the sample to cognitively intact nursing residents
Journal of elder abuse & neglect
Generalizablerandomsamplestudy
The average age of nursing home residents was 83.8 years. About 28% were male and 72% female. While 36.5% of respondents reported that a family member in a nursing home experienced staff abuse last year, only 10% reported non-personal abuse. In terms of health conditions, about 15.5% of nursing residents had a psychiatric diagnosis, 22.2% had behavioral problems and 85.3% had cognitive deficits. For physical functioning, there were 21.5% of respondents who could not perform any of the functional ADLs, and only 7.9% could perform the six ADLs.We identified five significant correlates of nonpersonal abuse reported by family members: behavioral problems, physical functioning, abuse by staff, gender, and age. Three of these correlates (physical functioning, behavioral problems and gender) were also identified as resident-to-resident aggression.Abuse of staff in nursing homes received much more public and academic attention compared to research focused on the incidence, prevalence, and risk factors for non-personal abuse.
Despite the strengths of our study, there are a number of limitations. First, although our estimate of nonpersonal abuse is based on reports from family members who may be close to effective for their frail elderly relatives in nursing homes. It is difficult to verify whether family members’ reports are more valid than institutional data sources. Second, due to the limitations of the research, we do not know the characteristics of the perpetrators (age, gender, health), perpetrating non-personal abuse (other residents or visitors), types of non- Physical abuse, verbal abuse, sexual abuse and the context of non-personal abuse. Thirdly, we have not been able to examine how the characteristics of nursing homes or nursing home staff (staff ratios, turnover, agglomeration) were associated with non-personal abuse. Fourth, all residents’ health problems have been reported by family members or responsible adults, some of whom may not have the most accurate information.
Our study shows that, according to family reports, 10% of nursing home residents aged 60 years or older in Michigan households experienced non-personal abuse in the past 12 months, while 36.5% experienced some type of abuse of staff. Further research is desperately needed in this neo-nascent field of elder abuse.
Schiamber et al.(2012)
This study included only 452 cases with elderly ≥ 65 years of age in a nursing home.
The study design was cross-sectional, with retrospective sequences from families with a family member in extended care.
Journal of elder abuse & neglect
Cross-sectional study
The incidence of physical abuse in nursing homes is described in two ways, the first being to use the number and percentage of individuals in the total sample (n = 452) who were abused (submitted to one or more of the three binary measures of global physical abuse). Using the binary variable strategy to measure the incidence of physical abuse, 110 elderly residents or 24.3% of the final analytical sample (n = 452) were submitted to physical abuse by nursing staff. The incidence of physical abuse is described by the type of physical abuse (the number and percentage of each of the three types of abuse in terms of the total amount of abuse). The frequencies and percentages of the total number of types of physical abuse for the three types of physical abuse are: physical mistreatment per team (hitting, hitting, kicking and so on), n = 44 or 27%; Constipation mistreatments, including inappropriate use of restrictions, forced toilet or unjustified forced feeding, n = 103 or 62%; Sexual abuse of the team, n = 18 or 11%. In our opinion, both measures of incidence are useful for understanding physical abuse in nursing homes.
That residents of nursing homes of Caucasian descent composed the main sample body (83%), the findings should not be considered as accurate reflections of experiences in more multicultural contexts. Although data collected in this study reflect the knowledge of family respondents about their older adult relatives in nursing homes, additional research is required to compare the results of this study with the survey using other forms of elder abuse reporting (eg, institutional self-report, criminal justice reports and government / agency data collection). Another limitation is that data were not collected on the characteristics and contexts of the institutional caregiver, an essential dimension of the focal context of physical abuse in the nursing home – the context of the elderly / institutional caregiver.
Physical abuse of nursing home staff occurs in the context of delivery of care efforts, suggesting the value of focusing on the adult-institutional elderly caregiver’s relational context as an initial context to frame the main characteristics of the relationship, including characteristics of the Adult older and caring staff.Finally, effective interventions to treat physical abuse of staff in nursing homes can be informed by the risk factors identified in this investigation, including in immediate and distal contexts.
Mistreatment
1
2
3
4
5
6
7
8Number Ofstudies 5 5 5 5 5 5 5 5
Shannon-Wiener Index0.3744 0.3053 0.4438 0.2403 0.3982 0 0 0.4297 Maximum Diversity 0.699 0.699 0.699 0.699 0.699 0.699 0.699 0.699 Homogeneity 0.5357 0.4368 0.6349 0.3438 0.5697 0 0 0.6148 Heterogeneity 0.4643 0.5632 0.3651 0.6562 0.4303 1 1 0.3852
Table 2 (above)
Legend: 1 – Physical abuse; 2 – psychological abuse; sexual abuse; 4 – abandonment; 5 – negligence; 6 – financial abuse; 7 – Invasion of privacy; 8 – verbal abuse.
Source: Evidence of articles.
Table 3.Reports of the main aggressors of the elderly living in long-stay institutions for the elderly.
Author/Year Title Objective Typeof agressor Grifforeetal..2009 Family members’ reports about nursing home abuse in Michigan. Describe the abuse and neglect of adults 65 years of age or older in Michigan homes as reported by family members. Respondents were asked if the person in the nursing home had experienced various types of abuse and neglect by staff or other caregivers in the past 12 months. The answer was that 73 (82% of those who responded to the item) reported at least one incident of maltreatment by staff (visitors) or caregivers (from the nursing home). Zhang et al.(2012) Reports from Family Members of Non-Personal Abuse in Nursing Homes in Michigan. Examine the abuse and exploitation of non-personnel perpetrators (residents, visitors, family members) in Michigan nursing homes. In this study, according to reports from family members, 10% of nursing home residents aged 60 and older in Michigan households have experienced non-personal (visitor or resident) abuse in the past 12 months; while 36.5% experienced some type of abuse of staff (staff). Borda &Yarnoz, (2015) Perceptions of abuse in care relationships in nursing homes in Uruguay. To describe care relationships between caregivers and elderly people in Uruguayan nursing homes. According to nursing home managers, discrimination arises among the elderly relative to their peers and from doctors to residents (seniors) about the care they provide. The types of elder abuse practices have also been detected by caregivers. Pillemer, et al. (2012) Resident-resident aggression in nursing homes: results of a qualitative study of reconstruction of events. Identify the main forms of ARR that occur in nursing homes. The analysis of 122 reconstructions of events identified 13 major forms of resident-resident aggression (RRA) grouped into five themes. The resulting picture demonstrated the heterogeneity of RRA types, the importance of considering personal, environmental and trigger factors, and potential emotional and physical damage to residents. Schiamber, et al.(2012) Physical abuse of the elderly in nursing homes: a random sample of adults with an elderly family member in an elderly household. To investigate the prevalence and risk factors of physical abuse of staff in elderly individuals receiving nursing care in Michigan. About 24.3% of the respondents reported at least one incident of physical abuse by the nursing team.
Figure 1 (PRISMA2009FlowDiagram).Identification and selection flowchart for articles for systematic review on elder abuse that remain in long-term institutions for the elderly.
Graph 1: Shannon-Wiener diversity index for ill-treatment of elderly people in Long-Term Care Facilities For the Elderly (below).
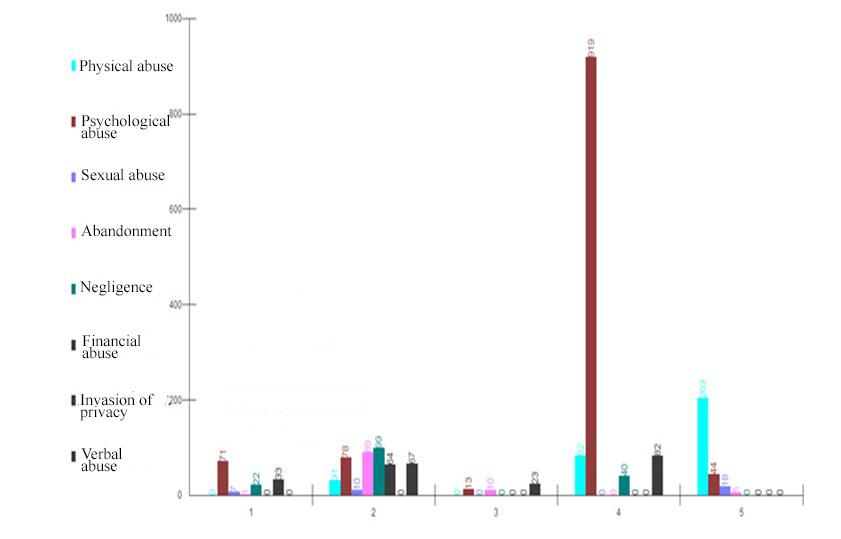
Graph 2: Distribution of samples of elder abuse in Long-term Institutions for the Elderly (below).
Graph 3: Density estimation for Physical-type mistreatment of elderly people in Long-Term Institutions for the elderly (below).
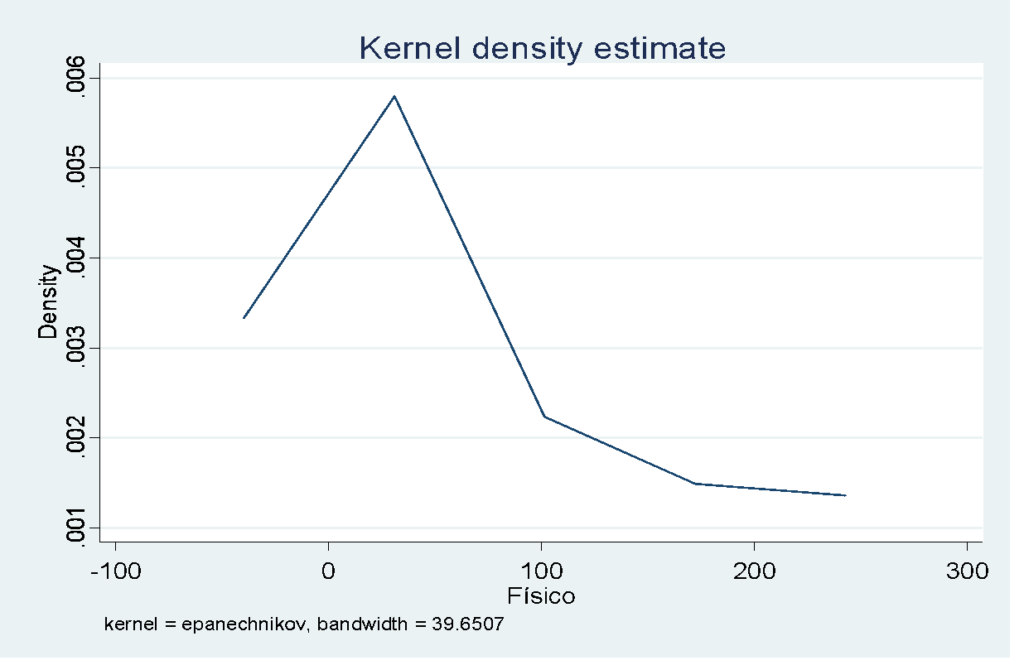
Source: Evidence from articles.
Graph 4: Density estimation for Emotional mistreatment of elderly people in Long-stay Institutions for the elderly (below).
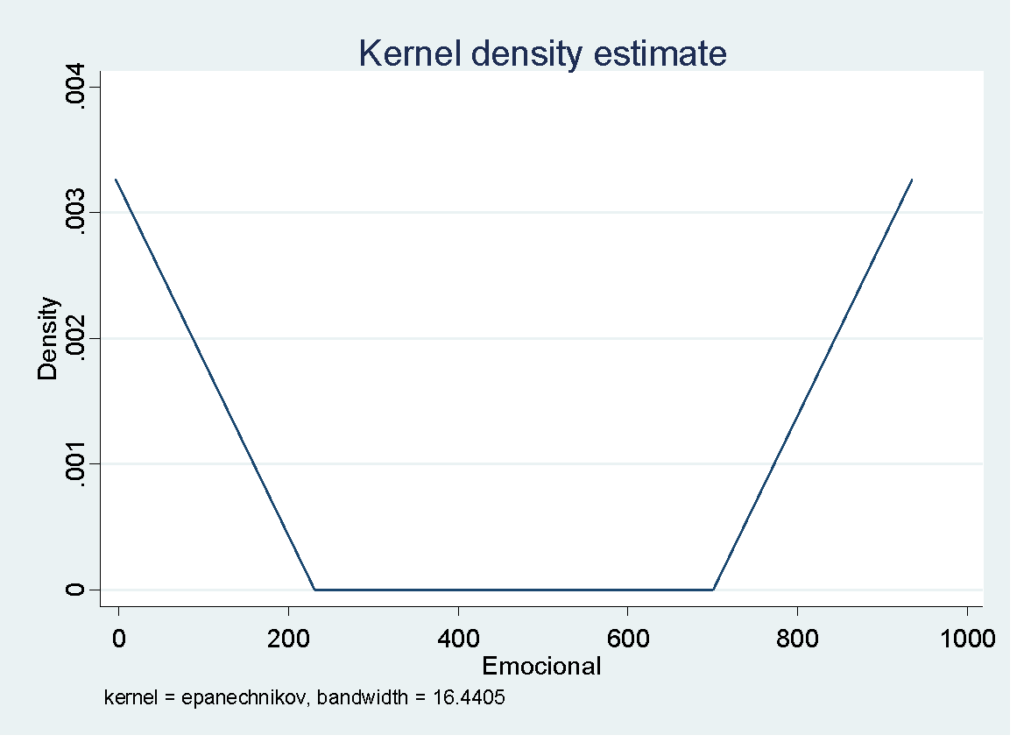
Source: Evidence from Articles
Graph 5:: Density estimation for mistreatment type of neglect of elderly people in institutions for long stay for the elderly.
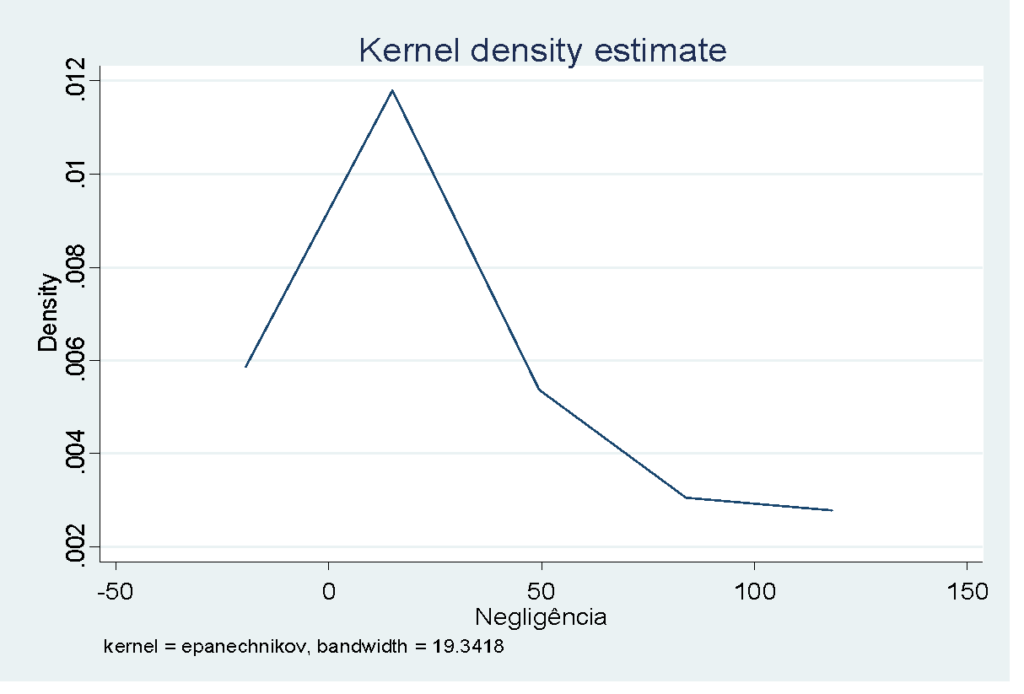
Source: Evidence from Articles
Graph 6: Density estimation for verbal mistreatment of elderly people in Long-Term Institutions for the elderly.
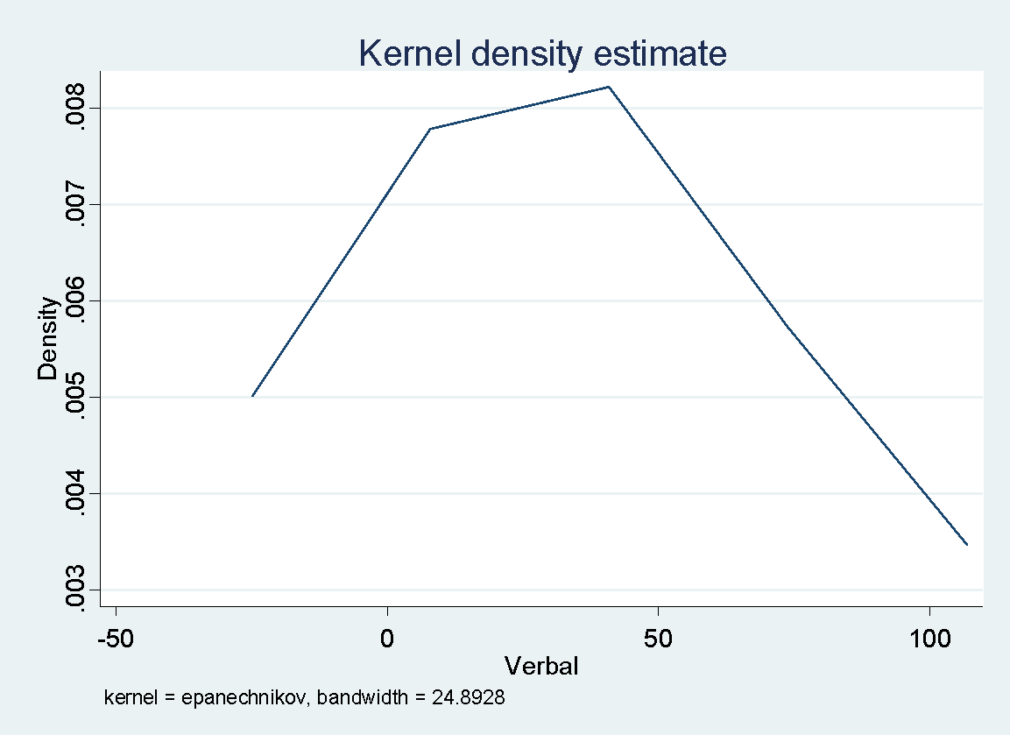
Source: EvidencefromArticles
1Fisioterapeuta, Mestre em Fisioterapia (Universidade Cidade de São Paulo – UNICID), Docente do Centro Universitario Doutor Leão Sampaio, orcid.org/0000-0003-3693-9864
2Fisioterapeuta, Especialista, Centro Univesitario Doutor Leão Sampaio, orcid.org/0000-000327887898
3Fisioterapeuta, Doutora em Saúde Pública (Universidade de São Paulo – USP), Docente na Universidade Federal de Sergipe, orcid.org/0000-0002-9782-4422
4Docente, Doutora em ciências da saúde (Centro Universitário Faculdade de Medicina do ABC, orcid.org/0000-0002-5504-4102
5Fisioterapeuta, Especialista em Saúde da Pessoa Idosa (Universidade Estadual do Ceara-UECE), orcid.org/0000-0003-3693-9864
6Nutricionista, Especialista, Universidade Federal de Sergipe, orcid.org/0000-0003-3886-4413
7Fisioterapeuta, Especialista em Dermato Funcional, Faculdade Uninta,
8Enfermeira, Especialista em Saude Publica, Faculdade Santa Emilia de Rodat