REGISTRO DOI: 10.69849/revistaft/ma10202306221402
Ana Vergínia Campagnollo Bueno1
Michelli Gonçalves Seneda1
Angela Mara Rambo Martini2
Ana Clara Campagnolo Gonçalves Toledo3
Caroline Cabral de Azevedo4
Adriane Viapiana Bossa5
ABSTRACT
Introduction: Obesity is a chronic disease that affects a large part of the population and can develop several outcomes such as cardiovascular disease, type II diabetes and some types of cancer. As a result, it favors negative aspects both for the individual and for the public administration. Faced with this problem, there is a need for new forms of treatment to improve the quality of life of these patients and reduce public spending. New alternatives to traditional medicine are needed to provide complementary non-drug treatments. Among them is Medicinal Biomagnetism (MB), a technique developed by Dr. Isaac Goiz Durán, which aims to favor the body’s homeostasis using medium intensity magnets. It is believed that this tool can act positively in the control, management and improvement of fluid retention in the body of obese individuals. Objective: This study aims to present and compile the MB 3D Protocol for the treatment of obesity with published evidence on Static Magnetic Fields (SMFs) applied to obesity treatment. Methodology: Qualitative, exploratory and descriptive literature review. Results: Some works were found demonstrating that MB therapy can benefit in obesity treatment. The 3D Protocol has therapeutic potential to produce positive effects, balancing the body’s homeostasis by helping metabolism regulation. Conclusion: Treatments with SMFs have beneficial effects on several aspects of obesity, which supports future studies that evaluate the results of the application of the 3D Protocol with this objective.
Keywords: Medicinal Biomagnetism; Magnetic Therapy; Protocol; Static Magnetic Fields; Inflammation; Obesity; Edema; Detoxification.
1. INTRODUCTION
The Ministry of Health in Brazil carried out a study to estimate the risk factors to protect chronic diseases that found obesity increased by 72% in the population over 18 years of age, going from 11.8% in 2006 to 20.3% in 20191.
This disease is a nutritional disorder of great impact in developed and underdeveloped countries. It is estimated that in 2025 at least 18% of the adult Brazilian population will be obese.
Obesity is considered an epidemic by many researchers. It is mainly related to the consumption of hypercaloric diets with a high content of saturated fat and sugars, present in the modern lifestyle, as well as the lack of physical activity2 leading to energy intake greater than body spending3. This growing incidence has tripled in recent years since 19753 and has become a public health problem due to the various diseases associated with it1.
The pathologies associated with obesity are: Acute Myocardial Infarction4, Stroke5,6, Diabetes Mellitus6, Chronic Kidney Disease and Hepatic Steatosis6,7. It is also associated with several types of cancer6,8, such as thyroid, esophagus, liver, gallbladder, colon and kidneys, as well as non-Hodgkin’s lymphoma and multiple myeloma9. It is believed that these outcomes are preceded by other factors, as obesity is complex and multifactorial7,10,11, involves metabolic factors12, increases insulin resistance and glucose intolerance13. Obesity produces a persistent chronic inflammatory state14 related to the accumulation of visceral fat, even considered as an inclusion factor for the Metabolic Syndrome (MS)2, which is characterized by a constellation of metabolic risk factors in an individual who presents the combination of at least three of the following components: waist circumference, triglycerides, HDL cholesterol, blood pressure and fasting blood glucose (according to NCEP III table – National Cholesterol Education Program Adult Treatment Panel III)15.
In this context, several therapeutic resources have been studied to reverse their morbidity and mortality impacts. Among the traditional and consolidated interventions, there are drugs that promote the suppression of hunger16, the practice of physical activity, as well as diets with different therapeutic approaches17.
The increasing statistics related to obesity, points toward the need for new forms of treatment to control this public health problem1 and improve these patients’ quality life. Complementary treatments to traditional medicine such as Medicinal Biomagnetism (MB)19 have been sought and are increasingly widespread around the world18.
The MB theory was developed in 1988 by the Mexican physician Durán19. It is a non-invasive complementary therapeutic system with minimal restrictions. This system works with static magnetic fields (SMFs), generated by medium intensity magnets (from 1000 to 7500 Gauss) with opposite polarities. It is agreed by the MB that the black color (negative) represents the north pole of the magnet and identifies points in excess of alkalinity, and the red (positive) represents the south pole and identifies points in excess of acidity19.
Magnets are applied to the body at specific polarized points. Polarization generates dysfunctional biomagnetic fields that remain in biomagnetic resonance, called Biomagnetic Pairs (BMPs), which cause distortions in the bioelectrical and biomagnetic balance and support dysfunctions and pathologies. This compromises body homeostasis that goes beyond the natural limits of organic entropy, the natural law that establishes health19. The SMFs depolarize the BMPs and, as consequence, the correction of homeostasis distortions occurs, helping the body to maintain the Normal Energy Level (NEL), in which maximum health is expressed19.
The construction of the MB theory was influenced by Broeringmeyer20, a NASA physician, who worked with SMFs. In cases of hypoactivity, the south pole of the magnet was applied and in cases of hyperactivity, the north pole of the magnet was applied to the affected organs, correcting the pH distortions, nullifying the opposite charge formed in the biomagnetic pole.
In MB, Biomagnetic Scanning (BS), performed with two magnets of opposite polarity, is the tool to carry out the diagnosis, treatment and prevention of various pathologies. Through scanning throughout the patient’s body in anatomical points already established, we search for BMPs that support pathologies. When applying the negative magnet (north pole) on the skin at some anatomical point with accumulation of negative OH- charges, in pH dysfunction, with greater alkalinity, shortening of the right hemibody occurs. Immediately afterwards, the point of magnetic resonance is sought, where there is accumulation of H+ ion, with greater acidity, the positive magnet (south pole) is applied on the skin and the members’ alignment occurs. Once the BMP is identified through the energy of the muscle test, the patient is treated with the negative magnetic pole on the first structure and the positive magnetic pole on paired structure19.
The magnets remain on the patient’s body for a period of 20 to 30 minutes to enable bipolar depolarization by magnetic repulsion. They push the pairs of charges in resonance to neutralize each other, balancing the bioenergetic field taking the organism to the Normal Energy Level (NEL) 19,21.
The magnetism generated by the magnets interferes with the body’s bioelectricity and this intervention influences the biochemistry (pH), restoring homeostasis. In this way, bioelectric restoration occurs in a specific body system or organ, favoring the adequacy of the local functioning of a group of cells and tissues, bringing benefits such as: endocrine and exocrine secretion, muscle tone, blood vessels, immune response, elimination of toxins and even cell regeneration when it is possible 21.
Some protocols were developed in the clinical practice of MB with the aim of enhancing the recovery of the body through specific BMPs for each dysfunction. They are auxiliary tools that can be used after a BS, as this is intended to act on the etiology of the signs and symptoms expressed in the body. Although easy to handle, they should only be used by professionals in the field22,23.
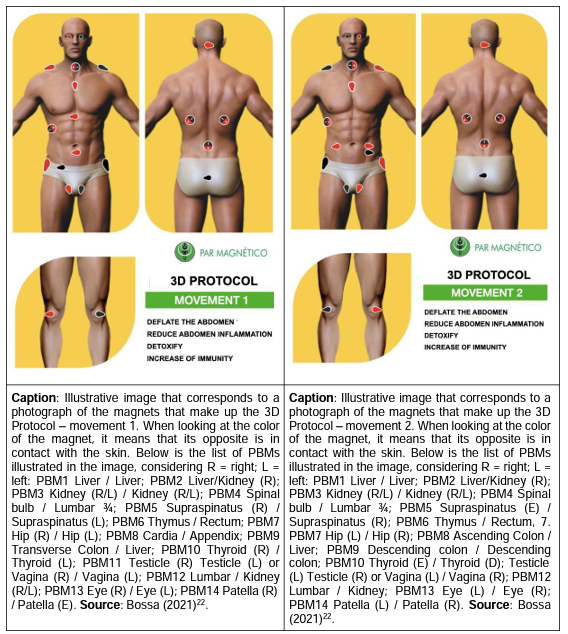
The “Basic – Personalized P1” and “Inverted P1” protocols created by Martínez23 were developed with the aim of detoxifying, reducing inflammation and deflate. Subsequently reformulated by Bossa22, called the 3D movement 1 and movement 2 protocol, it is a complementary tool to the BS, aiming to enhance the remission of obesity-related processes22,23. The magnets are represented on the BMPs of movement 1 and movement 2 are indicated in the images and described in the caption of Table 1:
Table 1: 3D Protocol – Movement 1 and Movement 2
This study aims to present and compile the MB 3D Protocol for the treatment of obesity with published evidence on SMFs applied in obesity.
2. METHODOLOGY
This is a qualitative, exploratory and descriptive literature review that consists of building a literature analysis with definitions from other authors, converging with the proposed objective of this study, which aims to present MB as a complementary practice in the treatment of obesity24.
The exploratory qualitative research allows an interaction between the theme and the authors since there is a lack of scientific literature on the subject to be discussed in the MB. In this context, proximity to the discussed subject and with the vast literature published on it is important, thus making it possible to explore the content to raise hypotheses that converge with the purpose of the study24.
The inclusion criteria for the theme of obesity and MB guided the literary search to select articles in full, in English, Spanish and Portuguese, prioritizing articles with Digital Object Identifier (DOI). The searches were carried out on Google’s Scholar basis chosen for its easy accessibility and scientific authenticity. The descriptors used to select the articles were obesity and Biomagnetism.
Surveys from public institutions dealing with problems related to obesity were also included. For the MB theme, due to the lack of publications converging with the objective of this study, the literature of the creator of the technique Dr. Isaac Goiz Durán and authors who follow his line, obtained from libraries of teaching institutions were selected. The literary search was based on books, articles, manuals, handouts from MB courses, theses and specialized studies on the theme.
For the description of the results, the material was submitted to exclusion criteria that considered articles published before 1997 with divergent content to the study topic of this research and duplicate articles. For the MB, the only exclusion criteria were works that were not related to the treatment of obesity.
The authors were responsible for searching, selecting and reading articles, books, manuals, theses and researches from selected public institutions, which contained all the written references for the theoretical basis of biomagnetism and obesity.
3. RESULTS AND DISCUSSION
As a result of the searches carried out in the electronic database of Google Scholar, according to the descriptors selected for the research, 148,010 documents were found on the theme of Biomagnetism and Obesity. After applying the inclusion and exclusion criteria, 30 documents were chosen for this study, 27 related to obesity, of which 14 without DOI, selected by proximity to the study, 3 related to Biomagnetism and 2 of them to MB. 13 documents obtained from a teaching institution’s library, 4 books, 4 manuals, 1 master’s thesis and 2 articles were included. Two publications from regulatory agencies were also selected, as summarized in Table 2.
Table 2: Search results in electronic databases
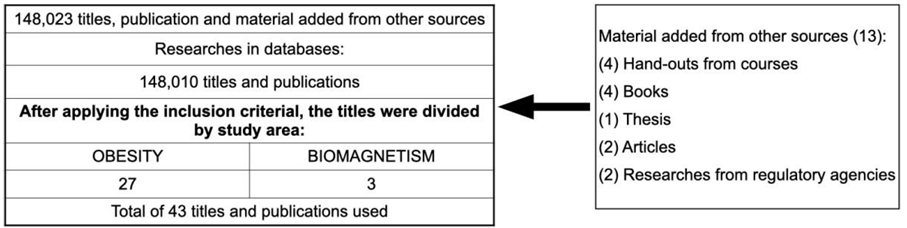
Source: The authors
From the acquired theoretical basis, the action of SMFs in obesity was related. In recent decades, the abdominal Adipose Tissue (AT) is no longer seen only as an energy store and has come to be identified as an endocrine organ for secreting substances classified as pro-inflammatory25. Excessive accumulations of AT can deregulate the endocrine system and inflammation factors in the body26, thus presenting abdominal circumference as an important clinical marker in the evaluation of obesity27 and an inclusion factor for Metabolic Syndrome28.
Inflammation in its general context occurs through the body’s metabolic and immune pathways aiming at homeostasis29, but the inflammation caused by obesity is known as dysfunctional inflammation30, consisting of adipocytes that produce pro- inflammatory cytokines31. Some of these mediators are responsible for inhibiting the signaling of insulin in muscle tissue, making glucose uptake slower32.
Insulin resistance in the blood, in turn, results in decreased glucose utilization and conversion of its excess into fat. Higher circulating triglycerides lead to excess fat in ectopic storage in the liver and arteries, in addition to increasing visceral fat accumulation33. Another important factor in this process is the characteristic of one of these inflammatory agents secreted by AT called Interleukin 6 (IL6), which in its high expression may be related to the suppression of leptin, the satiety hormone, which generates even more need for calorie intake by the body34.
Elevated levels of these inflammatory mediators produced by AT also stimulate the production of Plasma C-Reactive Protein (PCR) by the liver25, which has the function of assisting in the resolution of acute conditions causing inflammation so that the body gets rid of antigens such as infections and injuries35. However, what happens with chronic inflammation are only discrete elevations36.
Every disease is manifested by hyperalkanility and hyperacidity of the organic tissues that occur due to the altered concentration of hydrogens and free radicals, reducing oxygen and producing acidity in the diseased area that compromises the bioelectric and biomagnetic balance20. Biological magnetic fields originate from the electric currents that run through body cells that have specific magnetic values37,38. In this way, the SMFs allow the current to pass completely, without impediments, through the body, reaching each cell within the magnet’s energy field, promoting depth in the treatment20. According to the MB theory, SMFs correct homeostasis distortions, helping the body to maintain a Normal Energy Level (NEL)19.
The action of the SMFs generated by the therapeutic magnets of the MB on the inflammatory processes occurs through the application of the north pole of the magnets on the BMPs, which are related to the digestive, neuroendocrine and immune organs. As a result, there is a stimulus that promotes the elimination of fluids, contraction of the vessels, increase in alkalinity in the region affected by the north pole of the magnets, increase in oxygen in the tissues and a decrease in hydrogen ions, responsible for the acidification process, causing the tissues to recover their normality19,20.
The north pole of a magnet applied to a point with excess of negative charges in the body has the capacity to push such charges, correcting the bioelectricity of local cells, while the action of the south pole of magnets on BMPs directly affects H+ ions. When applied to the BMP, south pole and north pole magnets in each of the related regions promote a depolarization of the biochemical charges, normalizing the bioelectricity of the cell membrane. As a result, the previously dysfunctional pH is balanced, allowing the physiological activity of the cells to return to its normal, bringing the body to homeostasis, which is the basis of the body’s health19,20.
When magnets are applied to a BMP, the charges are pushed together by both polarities of the magnets and collide in some anatomical region, generating water. The water molecules in excess will be lead to excretion mainly through renal pathways 19, corroborating for the detoxifying and draining effect. There is still the action of the north pole of the magnets on the venous and lymphatic circulation since these impel the fluids as if pushing the transit of the flows. Such contraction, in addition to pushing the blood towards the right atrium, causes the blood flow to resume its course, increasing the delivery of oxygen to the tissues, resuming nutrition and cell function. With this, tissue function is restored19.
Since obesity is a systemic disease, which can be related to fluid retention, metabolism residues and systemic inflammatory agents, the application of the MB 3D Protocol is systematically presented to complement obesity treatment with the aim of deflating, reducing inflammation and detoxifying the body22,23 through SMFs that can correct the body’s bioelectricity, pH dysfunctions and balance the metabolism19, 20, 21.
The 3D Protocol requires the use of 28 magnets applied to different anatomical points that form the BMPs. The anatomical regions that receive the magnets are key points for the treatment of obesity that converge in MB literature19, 21,22, 23, 39, 40, 41, 42.
A study that associated acupuncture with MB obtained a better result in the treatment of obesity when compared to the treatment that only carried out acupuncture, thus indicating that MB can potentiate the beneficial effects for obese patients by acting directly on the balance of the body’s pH43.
In the theoretical bases on the causes of obesity, it was verified that the outcomes related to it involve endocrine, digestive and excretory systems, the latter being important in the role of detoxification. These systems are contemplated in the 3D Protocol and there are other literatures on the MB theme that promote the foundation of its use19, 23, 39.
The thyroid secretes and paces biochemical activity in the body. Under physiological conditions, the more hormones in their receptors, the faster the chemical activity, the less, the slower. All cells in the body are affected by the hormones produced by the thyroid19. The 3D protocol modulates the functioning of this gland, stimulating the body to deflate and detoxify39.
In the diagnosis of cancer, diabetes or any other disease such as obesity, there is a disorder in the cellular functions of tissues involving increased energy expenditure. The body creates electrical patterns to allow the patient to survive these conditions by expressing symptoms. In this way, the organism adapts to the electrical pattern altered by the pathological condition to survive in the face of the imposed circumstances. In this condition, the SMFs generated by the magnets act on the BMPs to normalize this energy and return to functional homeostasis through the production of antibodies to correct the existing problems22, 23. Thus, biological systems, including microorganisms, are affected by magnetic fields, in all the aspects19.
In a study carried out by Pirrone40 that presents a clinical case of Diabetes Mellitus treated with allopathy for 12 years without success, it demonstrates that after treatment with MB the patient started to have tests with normal glycemic levels. As obesity is related to insulin resistance, the magnets on the BMPs points used in this protocol can help in its regulation. There are also studies that demonstrate that MB associated with potentiated insulin therapy (PIT) proved to be beneficial in the treatment of metastatic cancer41, 42 thus sustaining that this treatment helps in reducing inflammation. Therefore, this technique can be used to prevent these types of outcomes from obesity.
The liver is responsible for more than a thousand biochemical functions in the body21 and when impacted by double magnets it helps in detoxification19, normalization of cholesterol, triglycerides, overweight and hepatic steatosis39. Still in the digestive system, we have some points of impact for the treatment of gastrointestinal dysfunctions22, such as malabsorption of the intestine, abdominal distension19, flatulence, protein food intolerance, fatigue39 and false diabetes (MB’s own term that relates to the symptoms of diabetes) 19.
The magnets in the kidneys help relax the renal arteries22, which in turn are responsible for the excretion of nitrogenous waste21 produced by metabolism, favoring homeostasis22.
In addition, the 3D Protocol works on other factors such as: regularization of the sympathetic and parasympathetic system, helps to relieve stress, improves glandular secretion, reduces muscle contraction, helps in the depolarization of other BMPs that may be active in the body, improves the effectiveness of medications22, strengthens the immune19 and respiratory39 systems, improving cellular oxygenation19. It also includes BMPs points that when treated can act beneficially on the psycho- emotional.
For these reasons, it is believed that magnetic therapy can contribute to the adjustment of the body to its electrical pattern in order to have maximum health20, thus justifying the use of the 3D Protocol for the treatment of obesity and prevention of its consequences.
Therefore, according to the compilation of studies selected for this review, among the articles published in scientific journals and sources of books and manuals specific to the subject, it is possible to believe that the 3D Protocol can promote benefits to improve the condition of obesity and its repercussions with the use of SMFs.
Other point that may justify and encourage the application of the MB according to Durán19 is the fact that the technique approaches the individual as a whole, being, for that reason, an alternative, complementary, non-invasive, low-cost therapeutic system that helps in the prevention, restoration and maintenance of health and well-being, balancing the body’s bioelectric and biomagnetic systems.
Systematically, the MB 3D Protocol must be applied by Biomagnetism therapists, who carry out the BS before its application, in order to enhance and personalize the effects of the treatment. For its application, the patient must be in a supine position. Movement 1 must be applied for 40 minutes and movement 2 for 20 minutes. The 3D Protocol must be applied in 10 sessions. The two movements (movement 1 and movement 2) must occur in the same session22, with a minimum interval of 7 days between each session. After the last application of the 3D protocol, wait 10 days and perform a new BS. The application of this process can be repeated as many times as necessary according to the therapeutic evaluation and desired results.
There is the possibility of customized application of the 3D Protocol. For this, it is recommended that the Biomagnetism therapist check the body for the required impaction time for each movement and the number of sessions between BSs. It is also important to point out that MB protocol does not replace a BS22, 23.
4. CONCLUSION AND PERSPECTIVES
This study presented the interrelationship between obesity and the action of SMFs generated by the MB therapeutic magnets, as well as a systematized form for the application of the 3D Protocol as a complementary treatment modality for obesity and its outcomes.
The lack of articles related to the MB presents a restriction to this study, limiting a more rigorous methodology in the parameters of inclusion of bibliographic references, although it did not compromise the significance of this research. It brings up the need for practical action on clinical studies related to MB that produce academic content.
Thus, the present research considers as a future perspective to study and evaluate the effects of the MB 3D Protocol in the format of a clinical trial so that evidence can be produced and presented.
REFERENCES
Claro RM, Monteiro CA, França GVA, Oliveira PPV, Gouvêa ECDP, Silva LES et al. Brasília DF Secretaria de Vigilância e Saúde. Vigilância de Fatores de Risco e Proteção para Doenças Crônicas por Inquérito Telefônico. Brasília. 2021.
Alves PHR, Corrêa CR. Relação entre Resposta Imune Inata do Receptor Toll- Like4 (TLR-4) e o Processo Fisiopatológico da Cardiomiopatia da Obesidade. Arquivos Brasileiros de Cardiologia. Botucatu. 2021; 117 (1): 91-99. doi: 10.36660/abc.20190788.
The World Health Organization [homepage na internet]. Obesity and overweight [acesso em 23 oct 2022]. Genebra. 2021. Available at: https://www.who.int/news- room/fact-sheets/detail/obesity-and-overweight.
Chew NWS, Kong G, Venisha S, Chin YH, Han NC, Muthiah M et al. Long-Term Prognosis of Acute Myocardial Infarction Associated with Metabolic Health and Obesity Status. Endocrine Practice. [place unknown]. 2022; 30 (5): 802-810. doi: 10.1016/j.eprac.2022.05.007.
Nchidzi N, Letamo G, Keetile M. Prevalence of and factors associated with hypertension, diabetes, stroke and heart attack multimorbidity in Botswana: Evidence from STEPS 2014 survey. [place unknown]. 2022; 24 (3): 1-16.
Veum VL, Borge JL, Eng Ø, Rostrup E, Larsen TH, Nordrehaug JR et al. Visceral adiposity and metabolic syndrome after very high–fat and low-fat isocaloric diets: A randomized controlled trial. The American journal of clinical nutrition. [place unknown].2017;105(1):85-99.
Ezequiel DG, Costa MB, Pinheiro HS. Obesidade: da fisiopatologia ao tratamento. HU rev. Juiz de fora. 2019; 44(2): 147.
Karra P, Winn M, Pauleck S, Jacobsen AB, Peterson Lacie, Coletta A et al. Metabolic dysfunction and obesity-related cancer: Beyond obesity and metabolic syndrome. [place unknown]. 2022;30(7): 1323-1334. doi: 10;1002/oby.23444.
Freitas C, Damasceno JL, Santos RA, Pina MGM. Obesidade e sua influência sobre o câncer: uma recente revisão da literatura. Revista de Atenção à Saúde. São Caetano do Sul. 2021;19(67): 344-356. doi: 10.13037/ras. vol19n67.7362.
Park SK, Jung JY, Oh CM, Choi JM, Kim MH, Ha E. Components of metabolic syndrome and their relation to the risk of incident cerebral infarction. Endocrine Journal. Japan. 2021; 68(3): 253-259.
Skilnik WL. Aprendizado de estruturas de dependência entre fenótipos da síndrome metabólica em estudos genômicos [dissertação]. São Paulo: Universidade de São Paulo, Faculdade de Saúde Pública; 2017 [citado 2022-10- 20]. doi:10.11606/D.6.2017.tde-04072017-105320.
Raposo HF, Basso LS, Delbue JL. Restrição alimentar de carboidratos no tratamento da obesidade. Rev. Ciênc. Méd. Campinas. 2012; 15(1): 56-67.
Maggio CA, Pi-Sunyer FX. The prevention and treatment of obesity. Application to type 2 diabetes. Diabetes Care. [place unknown]. 1997; 20(11): 1744 – 1997.doi: 10.2337/diacare.20.11.1744.
Cao W, Zhang T, Feng R, Xia T, Huang H, Liu C, Sun C. Hoxa5 alleviates obesity- induced chronic inflammation by reducing ER stress and promoting M2 macrophage polarization in mouse adipose tissue. J Cell Mol Med. China. 2019; 23(10):70297042. doi: 10.1111/jcmm.14600.
Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (adult Treatment Panel III), Final Report. Estados Unidos. The Program. 2002: 1 -293.
Fanghänel G, Cortinas L, Reyes S, Beber A. A clinical trial of the use of sibutramine for the treatment of patients suffering essential obesity. International journal of obesity. [place unknown]. 2000; 24 (2):144-150. doi:10; 1038/sj.ijo.0801098.
LI Jinghua. Effects of balanced diet associated with sports on the health of obese university students. Revista Brasileira de Medicina do Esporte. [place unknown]. 2022; 22(1): 1-4. doi: 10.1590/1517-8692202329012022_0183.
Kristoffersen AE, Broderstad AR, Musial F. Prevalence, and health-and sociodemographic associations for visits to traditional and complementary medical providers in the seventh survey of the Tromsø study. BMC complementary and alternative medicine. [place unknown]. 2019; 19 (1): 1-11.
Durán IG. El Par Biomagnético. Chapingo, México D.F. Universidad Autonoma Chapingo. México. 2008; (5): 2-177.
Broeringmeyer R. Principios de La Terapia Magnética. Bio- magnestismo. Health Industries, Inc. [place unknown]. 1991: 3-25.
Martinez DG. Manual del Biomagnetista. Ciudad de México: Biomagnetism Research Institute. Cidade do México. 2019.
Bossa AV. Biomagnetismo Medicinal Avançado, Bioenergética e Desbloqueio Emocional Magnético Avançados. Cascavel – Paraná. Fevereiro-2020; (1): 3-281.
Martínez DG. Protocolos de Biomagnetismo Minibook. Biomagnetism Researh Institute. Cidade do México. 2019: 1–131.
Gil AC. Como elaborar projetos de pesquisa. São Paulo: Atlas 1991.
Miraglia F, Mello ED. Como avaliar o processo inflamatório em crianças com excesso de peso?. Clin Biomed Res. Rio Grande do Sul. 2012; 32 (3): 332-339.
Kim EH, Kim HK, Lee MJ, Bae SJ, Choe J, Jung CH, et al. Sex differences of visceral fat area and visceral-to- subcutaneous fat ratio for the risk of incident type 2 diabetes mellitus. Korean Diabetes Journal. Korea. 2022; 46(3):486-498.
Li Shuying, Li Shaoping, Ding J, Zhou W. Visceral fat area and body fat percentage measured by bioelectrical impedance analysis correlate with glycometabolism. BMC Endocrine Disorders. China. 2022; 22 (1): 1-8.
Freitas ED, Fernandes AC, Mendes LL, Pimenta AM, Meléndez GV. Síndrome metabólica: uma revisão dos critérios de diagnóstico. Rev. Min. Enferm. [place unknown].2008; 12(3): 403-411.
Garias RD, Teixeira KM, Lagunes A. Programação bioenergética aplicada. [place unknown]. 2022; (4) 3-130.
Van de Velde F, Ouwens DM, Batens AH, Van Nieuwenhove Y, Lapauw B. Divergent dynamics in systemic and tissue-specific metabolic and inflammatory responses during weight loss in subjects with obesity. Cytokine. [place unknown]. 2021 v.144:155587. doi: 10.1016/j.cyto.2021.155587.
Alves PHR, Ferron AJTF, Costa MRC, Hasimoto FK, Gregolin CS, Garcia JL et al. Relação entre Resposta Imune Inata do Receptor Toll-Like-4 (TLR-4) e o Processo Fisiopatológico da Cardiomiopatia da Obesidade. Arq. Bras. Cardiol. [place unknown]. 2021; 117 (1): 91-99. Doi:10.36660/abc.20190788.
Effting PS, Brescianini SMS, Sorato HR, Fernandes BB, Fidelis GSP, Silva PRL et al. Exercício Resistido Modula Parâmetros de Estresse Oxidativo e Conteúdo de TNF-α no Coração de Camundongos com Obesidade Induzida por Dieta. Arquivos Brasileiros de Cardiologia. [place unknown]. 2012; 112(5): 545-552. Doi: 10.5935/abc.20190072 .
Kelly DM, Akhtar S, Sellers DJ, Muraleedharan V, Channer KS, Jones TH. Testosterone differentially regulates targets of lipid and glucose metabolism in liver, muscle and adipose tissues of the testicular feminised mouse. Endocrine. [placeunknown]. 2016; 54(2):504-515.
Souza EFG, Reis BGS, Brito ANM. O papel do adipócito na inflamação e metabolismo do obeso. Research, Society and Development. [place unknown]. 2021; 10 (9):1-10. Doi: 10.33448/rsd-v10i9.18191.
Pereira J, Cesca D, Daronco LSE, Balsan LAG. Efeito do tratamento quiroprático na concentração sérica de proteína C-Reativa e nos sintomas de indivíduos com cervicalgia. Salusvita, Bauru. 2016; 35 (2): 243-257.
Brasil AR, Norton RC, Rossetti MB, Leão E, Mendes RP. C-Reactive protein as an indicator of low intensity inflammation in children and adolescents with or without obesity. Jornal de pediatria. [place unknown]. 2007; 83(5): 477-480. Doi: 10.2223/JPED.1690.
Araújo DB de, Carneiro AAO, Moraes ER, Baffa O. Biomagnestismo: a nova interface entre a física e a biologia. Ciência Hoje. Rio de Janeiro. 1999; 26(153): 2433.
Perez IPD. O Efeito da Exposição de Campos Magnéticos Estáticos sobre Fibroblastos em Cultura. UFRJ, Rio de janeiro. 2022. Programa de Pós-Graduação Multidisciplinar em Física Aplicada.
Bossa AV. Protocolo de Rastreio do Biomagnetismo Medicinal. Instituto Par Magnético. Cascavel – Paraná. Outubro – 2022; 1(5) 3-122.
Pirrone IYO. Caso clínico de diabetes mellitus tratado con biomagnetismo médico. Segunda parte. [place unknown].
Damyanov C, Maslev I, Pavlov V, Todorov A. A New Treatment Method of Advanced Metastatic Tumors. Ann Clin Case Rep. 2019; (4): 1647.
Damyanov C, Maslev I, Pavlov V, Todorov A. Integrative Oncology at the Clinicist’s Look Chronology for the Creation and Development of the IPT & BMP Method for Treatment of Oncological Diseases. Clin Oncol. Bulgaria. 2019; (4): 1671.
Parra IA. Centro de Enseñanza de la Medicina Tradicional China. Estudio comparado de la aplicación de diferentes técnicas – acupuntura y biomagnetismo – en el tratamiento efectivo de la obesidad. Caracas. 2020; 2-109.
1Graduate specialists in Applied Biomagnetism and Bioenergetics for Health, Par Magnético Institute – IPM / Faculty of Governance, Engineering and Education of São Paulo – FGE, Brazil.
2Co-supervising Professor Program in Biomagnetism and Bioenergy Applied to Health, Par Magnético Institute – IPM / Faculty of Governance, Engineering and Education of São Paulo – FGE. SP, Brazil.
3Collaborating Professor of the Graduate and Master’s Program in Health Sciences of the
University of the West Paulista UNOESTE, Presidente Prudente-SP, Brazil
4Collaborating Professor – Master in Health Sciences by the Department of Psychiatry and
Medical Psychologist at EPM/UNIFESP
5Advising Professor Program in Biomagnetism and Bioenergy Applied to Health, Par Magnético Institute – IPM / University Center of Technology of Curitiba – UNIFATEC, Paraná, Brazil.