REGISTRO DOI: 10.69849/revistaft/cs10202505120017
Felipe Oliveira Saboya
Thiago Silva Alves de Oliveira
Matheaus Oliveira da Costa
Artur da Costa e Silva Craveiro
Vitor de Assis Cunha
Marcos William Cabral Silva
Samara Sousa Vasconcelos Gouveia
ABSTRACT
Introduction: Blood Flow Restriction Training consists of practicing physical exercises with partial restriction of blood flow. Significant muscle hypertrophy and strength adaptations can be achieved using light external loads. This effect has been observed in several clinical populations with load limitations. However, there are still uncertainties in the literature about the effects of this technique in patients undergoing rehabilitation after Anterior Cruciate Ligament Reconstruction. Objectives: To analyze the effects of the vascular occlusion technique on the lower limbs in patients undergoing rehabilitation after Anterior Cruciate Ligament Reconstruction. Methods: This is an integrative review, with searches performed in the PubMed, Scopus and Embase databases using the English descriptors blood flow restriction therapy; anterior cruciate ligament; resistance training and their variations in the same language, connected through the Boolean operator AND. Articles that referred to the topic addressed and/or related themes in full and publications in Portuguese or English were included, and incomplete texts and those that were not available in full were excluded. Result and Discussion: Ten manuscripts were selected for full analysis. Four publications demonstrated benefits related to increased muscle strength, four demonstrated improvement in atrophy or preservation of muscle mass volume, and three articles discussed improvements in pain perception. Conclusion: The technique of blood flow restriction therapy in post-surgical rehabilitation of the anterior cruciate ligament has shown promising potential regarding strength improvement, atrophy reduction and of pain relief. However, there is still a lack of protocols that can guide the indications of this therapy.
Keywords: blood flow restriction therapy; anterior cruciate ligament; resistance training.
INTRODUCTION
The anterior cruciate ligament (ACL) is an important component of the knee responsible for limiting varus and valgus stresses, hyperextension and preventing anterior translation of the tibia in flexion, in addition to providing stability to the knee. It originates anteriorly to the intercondylar eminence of the tibia, on the lateral surface of the medial tibial plateau, and inserts on the medial surface of the lateral femoral condyle, following a superior-posterior path (SACCO; TANAKA, 2008).
Abnormal anterior-posterior displacement movements of the tibia relative to the femur are referred to as drawer movements. In cases of ACL rupture or injury, the tibial displacement is anterior, resulting in a positive anterior drawer sign. The typical mechanism of ACL injury involves a combination of valgus stress, lateral rotation of the femur in a closed kinetic chain, and knee flexion—movements frequently observed in sports activities during pivots and directional changes with a fixed foot (SACCO; TANAKA, 2008).
The injury occurs when the ligament is stretched beyond its elastic capacity, and can be classified into three grades according to the extent of the rupture. A grade 1 injury occurs when there is a slight ligament injury with maintenance of the joint stability. In a grade 2 injury, a partial rupture of the ligament fibers occurs, resulting in ligament laxity. A grade 3 injury involves a complete rupture of the ligament structure, thus generating instability (PINHEIRO; SOUSA, 2015).
Studies indicate that ACL injuries are more common among individuals who engage in sports activities, especially at a professional level. Lima, et al (2020) demonstrated that knee injuries, including ACL injuries, are the fifth most frequent type of injury in soccer.
Global epidemiology on the subject is well-documented. According to Pinheiro and Souza (2015), in Germany in 2015, the incidence of ACL ruptures in the general population was 30 cases per 100,000 inhabitants and around 70 cases per 100,000 among athletes. Similarly, according to the authors, the United States recorded around 200,000 ACL injuries, of which 100,000 required surgical treatment.
The diagnosis is based on clinical history, physical examination and imaging studies. Patients with ACL injuries present pain, edema, redness, loss of range of motion and a sensation of knee instability. Tests are always performed bilaterally, compared with the healthy knee. The Lachman, Pivot Shift, Mac-Intosh and Anterior Drawer tests can be used in clinical practice (PINHEIRO; SOUSA, 2015).
Several techniques are employed for Anterior Cruciate Ligament Reconstruction (ACLR) such as autografts using the quadriceps tendon, hamstring tendons, and allograft materials. The gold standard is the patellar tendon autograft, which involves arthroscopy for graft harvesting, graft preparation, intercondylar notchplasty, drilling of tibial and femoral tunnels, graft passage, and femoral and tibial graft fixation (SCOTT, 2019).
Muscle atrophy and weakness are common in patients undergoing anterior cruciate ligament reconstruction, and efforts to minimize these effects are a challenge in the treatment of this surgery. Strength development depends on the external load exerting traction on the muscle and the number of repetitions performed, in which, to achieve hypertrophy, a load <60% and repetitions between 8 and 12 would be required. However, training at this intensity soon after anterior cruciate ligament reconstruction stresses the damaged tissues, delaying the healing process and prolonging rehabilitation time (LORENZ et al., 2021).
This highlighted the need for a technique capable of providing low-intensity training, while producing positive effects on muscle strengthening, using lower loads, with repetitions until failure, to minimize excessive stress on healing tissues, without compromising effectiveness compared to conventional strength training.
Blood Flow Restriction Training (BFRT) is synonymous with terms such as Kaatsu (Kaatsu Global, Inc), flow occlusion training, and hypoxic training. The test is performed using a cuff to promote partial occlusion of the affected limb. The loads achieved in training are generally lower (20% to 30% of 1-RM; 15 to 30 repetitions per set) due to the low blood supply oxygenating the muscle during the test, consequently leading to fatigue more quickly (LORENZ et al., 2021).
Therefore, there is optimism regarding the applications of the technique, as numerous studies are being conducted on the subject. Despite using lower loads, BFRT generates a high perception of effort while preserving surgical sites and reducing shear forces. However, there are still uncertainties in the literature about the effects of this technique in patients undergoing ACLR.
GENERAL OBJECTIVE
To analyze the effects of the vascular occlusion technique on the lower limbs in patients undergoing rehabilitation after Anterior Cruciate Ligament Reconstruction.
METHODOLOGY
Seeking to answer the guiding question: “What are the effects of vascular occlusion in the lower limbs in patients undergoing rehabilitation after anterior cruciate ligament reconstruction”, the methodological approach for this study was conducted through an Integrative Literature Review, a scientific methodology that provides relevant subsidies for strengthening Evidence-Based Practice. (Mendes; Silveira; Galvão, 2008);
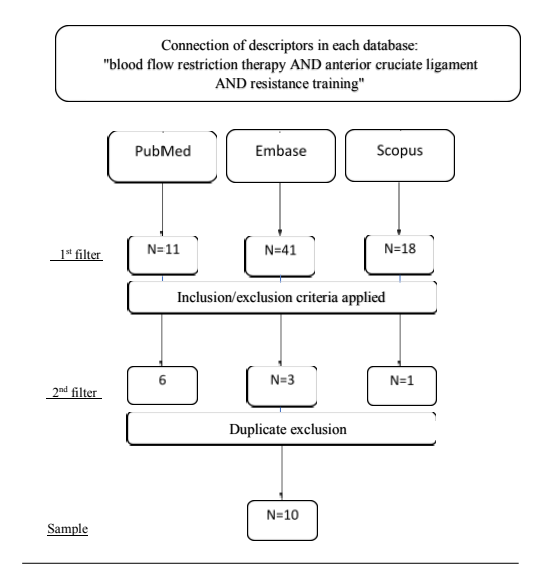
The manuscripts were selected from the PubMed, Embase and Scopus databases, using the following combination of descriptors: “blood flow restriction therapy AND anterior cruciate ligament AND resistance training”. Then, the literary stratification occurred based on the delimitation of the inclusion criteria that met study’s objective, which included: articles addressing the topic and/or related themes in full and publications in Portuguese or English. Incomplete texts and those that were not available in full on the internet were not included as exclusion criteria. As a final filter, duplicate publications were analyzed to refine the sample for exploration. The time frame followed the selection of texts published in the last five years (Figure 1).
Data analysis and organization were performed using tables and charts from our own sources, grouped according to the following variables: author/year, study design/level of evidence, and results. The results and discussions were presented based on the prevalence categorization highlighted by the articles, considering the importance and relevance of the data through a hierarchical analysis of the studies and their research designs, a method that helps the visualization of the publications evidence levels.
Figure 1. Databases searched and selected articles.
RESULTS
Throught the screening process, 70 potentially eligible articles were identified based on a quick review of the title, objective(s) and year of publication. Of this total, 10 manuscripts were fully analyzed through a thorough and systematic reading. To achieve greater clarity regarding the textual approaches and dynamics in the understanding of each analyzed article, a distribution was proposed to highlight the key aspects addressed by each publication.
Table 1 – Distribution of studies according to article title and year of publication.
| N | Title | Author(s) | Year of Publication |
| 1 | Surgical versus conservative interventions for treating anterior cruciate ligament injuries | Monge et al | 2016 |
| 2 | Blood Flow Restriction Therapy Versus Standard Care for Reducing Quadriceps Atrophy After Anterior Cruciate Ligament Reconstruction | Lipker, et al | 2019 |
| 3 | Effect of Blood Flow Restriction Training on Quadriceps Muscle Strength, Morphology, Physiology, and Knee Biomechanics Before and After Anterior Cruciate Ligament Reconstruction: Protocol for a Randomized Clinical Trial | Erickson et al | 2019 |
| 4 | Blood Flow Restriction Training Applied With High-Intensity Exercise Does Not Improve Quadriceps Muscle Function After Anterior Cruciate Ligament Reconstruction: A Randomized Controlled Trial | Curran et al | 2020 |
| 5 | Rehabilitation with the aid of blood flow restriction training | Rolff; korallu s; hanke, | 2020 |
| 6 | Rehabilitation outcomes and parameters of blood flow restriction training in ACL injury: A scoping review | Caetano et al | 2021 |
| 7 | Blood Flow Restriction Training Can Improve Peak Torque Strength in Chronic Atrophic Postoperative Quadriceps and Hamstrings Muscles | Noyes; Barber Westin; Sipes | 2021 |
| 8 | Influence Of Blood Flow Restriction Training on Knee Pain After Anterior Cruciate Ligament Reconstruction: A Double Blinded Randamized Controlled Trial | Khalil et al | 2023 |
| 9 | Comparison of Blood Flow Restriction Interventions to Standard Rehabilitation After an Anterior Cruciate Ligament Injury: A Systematic Review | Colombo etal. | 2024 |
| 10 | The Effectiveness of Blood Flow Restriction Technique Combined with Low-Resistance Exercise in the Postoperative Rehabilitation of Patients Following Knee Surgery: A Narrative | Limbari et al. | 2024 |
Another important categorization employed in the study was the classification of the manuscripts based on their level of evidence. This approach allows a methodological assessment of how the topic is addressed in the literature. Therefore, given the wealth of publications analyzed, the level of evidence for each article was explicitly presented to ensure credibility and emphasize the reliability of the findings.
Table 2 – Distribution of studies according to results, study design, and level of evidence
| N | Main Results | Study Design | Level of Evidence |
| 1 | A study with 36 participants, including both men and women, showed no significant differences (p value > 0.05) between group (A) CRP and group (B) BFR added to CRP when knee pain was assessed using the VAS scale. | Double-Blind Randomized Trial | Level II |
| 2 | The literature search identified 279 studies, of which 5 met the selection criteria. Two studies suggested that using BFRT rehabilitation after an ACL injury improved knee or thigh muscle strength and muscle size, while two studies suggested otherwise. | Systematic Review | Level I |
| 3 | Additional data are needed to determine whether the benefits of BFRT in addressing quadriceps atrophy after ACL reconstruction outweigh the inherent risks and costs. | Randomized Clinical Trial | Level II |
| 4 | BFRT combined with high-intensity resistance exercise added to an ACL rehabilitation program did not significantly improve strength recovery. | Randomized Clinical Trial | Level II |
| 5 | Twenty-seven patients (18 women, 9 men; mean age 40.1 years) with severe quadriceps and/or hamstring deficits were enrolled from April 2017 to January 2020. All patients completed 9 sessions of BFRT, and 14 patients completed 18 sessions. | Prospective Study | Level II |
| 6 | Three out of four studies demonstrated an increase in the cross-sectional area of the femoral muscle after the use of BFR combined with low-intensity resistance training. | Scoping Review | Level IV |
| 7 | A total of 7 articles were deemed eligible and utilized BFRT in surgical rehabilitation. Muscle size was assessed in all studies, and most also evaluated muscle strength (71%; n=5). Only one study assessed physical functional outcomes. Additionally, only one study (14%) examined the efficacy of BFRT without training. The evidence remains scarce and insufficient due to the heterogeneity of the reported outcomes. | Systematic Review | Level I |
| 8 | BFR and resistance exercise may be effective in improving patient outcomes after knee surgery. However, further studies are needed to identify the optimal dosage, frequency, and duration of BFR and low-resistance exercise for knee surgery rehabilitation. | Integrative Review | Level IV |
| 9 | In postoperative treatment following knee arthroscopy and anterior cruciate ligament reconstruction, BFR can be utilized to reduce atrophy. | Systematic Review | Level I |
| 10 | Primary Outcome: Quadriceps peak force and rate of torque development measured symmetrically and isokinetically. Secondary Outcome: Knee biomechanics, quadriceps muscle morphology, and physiology. | Double Blind Randomized Trial | Level II |
Once the core focus of each article was analyzed, the predominant categorical variables identified were muscle strength, muscle hypertrophy, and perceived pain improvement. In general, few manuscripts described more than one variable, which limited the analysis of each publication to just one variable in most cases. However, the validations of each category in each study are emphatic regarding the results, allowing independent analysis without the need for comparison.
Regarding the variable muscle strength, 41.6% of the studies reported an increase in strength when flow restriction therapy was used. Regarding muscle hypertrophy, 33% of the publications indicated a reduction in muscle atrophy as well as an increase in muscle cross-sectional area. As for pain perception, 25% of the studies addressed this aspect in their results, however, only 16.6% showed a reduction in pain perception with the use of this therapy, while 8.33% found it to be indifferent when analyzing this variable.
It is worth highlighting that, overall, when analyzing the entirety of the publications (10), 25% of them showed no difference in the effectiveness of the flow restriction therapy in any of the categories analyzed, that is, they were indifferent to the observed approach.
Table 3 – Quantitative Distribution Regarding Muscle Strength, Muscle Hypertrophy, and Pain Perception
| Study | Muscle strength | Muscle Hypertrophy | Pain Perception |
| 1 | Increased | Not described | Improved |
| 2 | Increased | Not described | Not described |
| 3 | Not described | Atrophy reduction | Not described |
| 4 | Not described | Not described | Not described |
| 5 | Increased | Atrophy reduction | Improved |
| 6 | Not described | Atrophy reduction | Not described |
| 7 | Not described | Not described | Not described |
| 8 | Increased | Atrophy reduction | Not described |
| 9 | Not described | Atrophy reduction | Not described |
| 10 | Increased | Avoided atrophy | Improved |
DISCUSSION
It is important to highlight that 20% of the studies included in the sample did not show significant relevance concerning the most commonly analyzed variables. This can be observed in the study by Curran et al. (2020), which demonstrated that blood flow restriction training applied with high-intensity exercise does not improve quadriceps muscle function after anterior cruciate ligament reconstruction.
Furthermore, Caetano et al. (2021) showed that the limited number of studies and the lack of standardization in BFRT prescription parameters hinder the comparison of results across different studies.
Monge et al. (2016) reported that BFRT, when applied during the perioperative period, can improve muscle function and reduce recovery time. However, the study emphasized the need for further research to establish consistent protocols and identify potential long-term risks associated with BFRT use in patients undergoing ACL surgery.
On the other hand, the central discussion supported by 80% of the manuscripts in the sample regarding the use of blood flow restriction therapy in the anterior cruciate ligament reconstruction process deals, in summary, with the variables muscle strength, muscle hypertrophy and pain perception in patients undergoing this type of treatment.
Evaluation of Muscle Strength
Considering the entire sample, muscle strength was mentioned in four publications (40%) with a similar assessment of the intervention effectiveness. This is shown in the study by Roff; Korallus; Hanke (2020), which investigated the effects of BFRT combined with low-load exercises compared to conventional rehabilitation in an assisted rehabilitation setting.
This study demonstrated that BFRT resulted in significant improvements in muscle strength recovery in post-operative ACL patients. Furthermore, the intervention showed efficacy in patients unable to perform high-load training, being considered an alternative for improving muscle function without increasing joint stress (Roff; Korallus; Hanke, 2020).
Similarly, in a comparative study of BTRF with standard rehabilitation after ACL injury performed by Colombo et al. (2024), it was possible to observe the superiority of BFRT over conventional therapy in aspects of muscle strength gain, especially when associated with low-intensity exercises. However, the authors reinforce the need for further studies on the long-term impact of BTRF.
There is broad consensus in the literature regarding the improvement of muscle strength after flow restriction therapy. Erickson et al. (2019) also highlights the effectiveness of BTRF in preserving muscle strength through a protocol showing the implementation of the therapy during the preoperative phase as well as the functional improvement in the postoperative period of patients undergoing ACL reconstruction.
Evaluation of Muscle Hypertrophy
According to 40% of the studies in the sample, blood flow restriction therapy also has a significant positive impact on muscle hypertrophy. BTRF has proven to be a valuable tool in the rehabilitation of patients with significant muscle atrophy after
ACL surgery. Noyes; Barber-Westin; Sipes (2021) evaluated the improvement in peak torque strength of atrophied quadriceps and hamstring muscles in the postoperative period.
Similarly, Colombo et al. (2024) demonstrated in their results that the application of BFRT in patients undergoing ACL reconstructive therapy led to significant gains in muscle hypertrophy despite the conventional technique. In this sense, flow restriction training allows a faster return to the individual’s standard of functionality, which reduces the rehabilitation time for these patients.
Lipker et al. (2019) corroborates the idea of shortened rehabilitation period, when they show, in a comparative study between BFRT therapy and standard care, the ability to reduce muscle atrophy after ACL reconstruction in a shorter period of time. The study also highlighted that BFRT therapy was effective in reducing quadriceps atrophy, providing significant gains in muscle function, offering a more efficient alternative for patients experiencing postoperative muscle mass loss.
In addition to improving the muscle trophic state and preserving muscle mass after using BFRT combined with low-resistance exercises, Limbari et al. (2024) demonstrated in their study, focused on updates in physiotherapeutic practices for postoperative rehabilitation of patients with knee injuries, that blood flow restriction therapy is safe when properly applied. The study highlights BFRT as an emerging practice in evidence-based physiotherapy.
Evaluation of Pain Perception
Within the process of categorizing variables, another aspect cited by 30% of the publications in the sample concerns pain perception after flow restriction training. According to Roff; Korallus; Hanke (2020), an assisted rehabilitation study utilizing BFRT found that the effects of BFRT combined with low-load exercises, compared to conventional rehabilitation, resulted in significant improvements in pain reduction in postoperative ACL patients. Additionally, this approach contributed to the prevention of joint stress in patients with contraindications for high-load training. In a similar analysis, Limbari et al. (2024) observed a reduction in pain during the recovery process of postoperative ACL reconstruction patients. Another key point highlighted by the authors is that BFRT demonstrated a good degree of safety when applied correctly, following established protocols, minimizing the risk of iatrogenic complications associated with the use of blood flow restriction training.
Still within this variable, other authors also support the validation of the method in reducing pain. This is evidenced by Khalil et al. (2023) through a double blind randomized controlled trial that sought to evaluate the influence of BFRT on knee pain after ACL reconstruction. The study revealed that patients who used BFRT experienced a significant reduction in pain compared to the control group, in addition to suggesting the technique as a promising tool for pain management and accelerating rehabilitation after ACL reconstruction surgery.
CONCLUSION
Therefore, it is evident from a comprehensive analysis that blood flow restriction training is capable of improving muscle strength and muscle hypertrophy, both in terms of reducing atrophy, preventing muscle mass loss, and promoting lean mass hypertrophy, in addition to presenting a beneficial effect in pain relief, reaching significant reductions in pain levels.
However, given the small sample size, further studies are needed to address the biases observed in the literature, especially regarding the applicability of the technique associated with low-intensity exercises, the absence of protocols for studying BFRT in specific injuries, the lack of parameters that enable comparisons across different studies and the potential risks associated with prolonged use of the therapy.
STATEMENTS:
Abbreviations
ACL Anterior Cruciate Ligament
ACL-R Anterior Cruciate Ligament Reconstruction
BFRT Blood Flow Restriction Training
Ethical approval and consent to participate
Not applicable, This is an integrative literature review.
Consent for publication
Not applicable. This is an integrative literature review.
Availability of data and materials
Obtained through digital platforms as detailed in the methodology.
Competing interests
There is no conflict of interest with this article.
Funding
None.
Authors’ contributions
Saboya and Nunes participated in the study design, data collection, data analysis, and manuscript drafting. Gouveia participated in the manuscript review and drafting.
REFERENCES
CURRAN, M. T. et al. O treinamento de restrição de fluxo sanguíneo aplicado com exercício de alta intensidade não melhora a função muscular do quadríceps após reconstrução do ligamento cruzado anterior: um ensaio clínico randomizado. American Journal of Sports Medicine, 2020.
CAETANO, D. et al. Resultados da reabilitação e parâmetros do treinamento de restrição de fluxo sanguíneo na lesão do LCA: uma revisão de escopo. Physical Therapy in Sport, 2021.
COLOMBO, V. et al. Comparação de intervenções de restrição do fluxo sanguíneo com a reabilitação padrão após uma lesão do ligamento cruzado anterior: uma revisão sistemática. 2024.
ERICKSON, L. N. et al. Efeito do treinamento de restrição do fluxo sanguíneo na força, morfologia, fisiologia e biomecânica do joelho do quadríceps antes e após a reconstrução do ligamento cruzado anterior: protocolo para um ensaio clínico randomizado. Phys Ther 2019.
KHALIL, A. A, et al. Influência do treinamento de restrição do fluxo sanguíneo na dor no joelho após reconstrução do ligamento cruzado anterior: um estudo controlado duplo-cego e controlado. Jornal de Terapêutica Populacional e Farmacologia Clínica 2023.
LIMBARI, M. et al. A Eficácia da Técnica de Restrição do Fluxo Sanguíneo Combinada com Exercício de Baixa Resistência na Reabilitação
Pós-Operatória de Pacientes Pós-Cirurgia do Joelho: Uma Revisão Narrativa e Atualização da Prática de Fisioterapia Baseada em Evidências. Revisões Críticas em Medicina Física e de Reabilitação 2024.
LIPKER, L.A. et al, Terapia de restrição do fluxo sanguíneo versus padrão Cuidados para reduzir a atrofia do quadríceps após o ligamento cruzado anterior reconstrução. JSport Rehabil. 2019
LOREZ, D. S. et al. Blood Flow Restriction Training. J Athl Train. 2021.
MONGE, A. P, et al. Intervenções cirúrgicas versus conservadoras para o tratamento de lesões do ligamento cruzado anterior. Sistema de banco de dados Cochrane Rev. 2016.
NOYES, F.R; BARBER-WESTIN, S. D; SIPES, L. O treinamento de restrição do fluxo sanguíneo pode melhorar o pico de força de torque nos músculos quadríceps e isquiotibiais atróficos crônicos. Artroscopia. Epub 2021.
PINHEIRO, A.; SOUSA, C. V. Lesão do ligamento cruzado anterior: apresentação clínica, diagnóstico e tratamento. Rev Port Ortop Traum. 2015.
ROLFF, S; KORALLUS, C; HANKE, A. A. Rehabilitation mithilfe des “blood flow restriction training” [Reabilitação com o auxílio de treinamento de restrição do fluxo sanguíneo]. Unfallchirurg. 2020.
SACCO, I. C. N.; TANAKA, C. Cinesiologia e Biomecânica dos Complexos Articulares. (Série Fisioterapia: Teoria e Prática Clínica) . [Digite o Local da Editora]: Grupo GEN, 2019. E-book. ISBN 9788527739429. Disponível em: https://app.minhabiblioteca.com.br/#/books/9788527739429/. Acesso em: 01 dez. 2023.
SCOTT, W N. Insall & Scott Cirurgia do Joelho . [Digite o Local da Editora]: Grupo GEN, 2019. E-book. ISBN 9788595157569. Disponível em: https://app.minhabiblioteca.com.br/#/books/9788595157569/. Acesso em: 04 dez. 2023.