REGISTRO DOI: 10.69849/revistaft/fa10202504132310
Guaracy Lyra da Fonseca Júnior1, Fabiana Souza dos Santos2, Ney Tavares Lima Neto3, Jorgiane Rodrigues Gurgel Lessa4, Nivaldo Antônio Bernardo de Oliveira5, Luiz Felipe Azevedo6
ABSTRACT
The growing demand for esthetic orthodontic treatments has driven the evolution of techniques in dental practice. In this context, the 3DBOT (Bracketless orthodontics treatments) technique emerges as an innovative and effective alternative. This technique, combined with skeletal anchorage devices, has proven effective in the treatment of Angle Class II malocclusion. The present article presents a case report on the correction of a Class II malocclusion without the use of brackets through the 3DBOT technique, assisted by orthodontic mini-implants and finalized with esthetic aligners. The objective is to demonstrate the effectiveness and esthetics of the treatment, meeting the patient’s expectations. It was concluded that the 3DBOT technique, combined with mini-implants and orthodontic aligners, proved to be highly effective in the correction of Class II malocclusion.
Descriptors: Angle Class II Malocclusion, Bracketless Fixed Orthodontics, Esthetics, Orthodontics.
INTRODUCTION
The search for orthodontic treatments is often associated with improvements in the function and esthetics of the smile. Class II malocclusion, for example, can significantly compromise dental esthetics, resulting in inclinations or retroclinations of the upper anterior teeth. The type of treatment indicated varies according to the anteroposterior discrepancy presented. 1,2,3
Strategies for correcting Class II malocclusion are varied, including tooth extractions, functional orthopedic appliances, orthognathic surgery, and distalizing appliances, both external and intraoral. However, patients have shown an increasing preference for less visible appliances. Lingual braces, for example, are an effective esthetic alternative since they are glued to the lingual surface of the teeth, although they can cause discomfort when the tongue adapts. In turn, aligners, widely used in clinical practice, have the disadvantage of losing part of their esthetics due to the need for attachments4,5
According to Fonseca JR (2023)2, virtual planning has proven to be an essential tool for correcting deformities and asymmetries that were previously difficult to resolve with conventional two-dimensional approaches. This technology also allows for the identification of possible complications and the optimization of mandibular positioning in the temporomandibular joints (TMJs).
Given this advancement in corrective orthodontics, the bracketless technique has stood out for not using brackets and for not interfering with speech, positioning 3DBOT as an excellent choice for patients. According to Fonseca et al. (2022)6, this modality of orthodontic treatment emerged as a response for the need to stabilize the anterior teeth, in addition to enabling controlled movement without the use of metal or ceramic brackets through the pre-activation of orthodontic wires.
The technique benefits from the use of 3D orthodontic movement software, providing predictability in treatment and meeting the esthetic demands of patients. Lima Neto et al(2022)7 reaffirms that the combination of the versatile skeletal anchorage plate in the palate with the 3DBOT technique represents a viable and effective option for the treatment of Class II malocclusion. The objective of the present article is to report a clinical case of Class II treatment with the 3DBOT technique and the aid of a mini implant in the infrazygomatic crest.
CASE REPORT
An 18-year-old male patient attended the oral esthetics clinic in Recife-PE, complaining of crowding in the upper and lower arches and “compressed arches.” Intraoral clinical examination revealed an Complete bilateral Class II malocclusion of 7 mm. Facial examination revealed a mesofacial pattern, a well-defined nasolabial angle, and a passive lip seal. Teleradiography confirmed accompanied by increased overjet and extrusion of the upper incisors. Intraoral photographs showed moderate crowding in both arches, in addition to the presence of a curve of Spee. Panoramic radiographs revealed the presence of impacted third molars and a nasal septum without deviation.
Based on clinical and radiographic data, intraoral scanning and digital planning were performed using the NemoCast software, correcting crowding and rotations, adjusting the midline and the relationships between the canines and molars, predicting completion with aligners. For the treatment, the 3DBOT device with 014 niti wire (Morelli) was installed in the upper and lower arches. Mini orthodontic implants (Morelli) were placed in the infrazygomatic crest region and esthetic buttons were installed on teeth 14 and 24 using Elink type elastics (TP Orthodontics), starting with a force of 150g. Due to relapses and detachment of the buttons, tubes were glued to teeth 36 and 46 for the use of Class II elastics, 3/16 medium.
The wires were replaced during the consultations, as were the E-link elastics. With the wire changes, crowding was reduced, the extrusion of the upper incisors was reduced and the midline was corrected. During the treatment, with the replacement of the elastics, the overhang was reduced and the molar and canine relationship was normalized to Angle Class I. After completing what was expected and planned for the 3DBOT, the patient advanced to the aligner phase (in office) of the My Aligner type. A new scan was performed, as well as a new planning for this phase, resulting in a total of 8 aligners for the upper arch and 6 for the lower arch. To facilitate the desired movements, upper and lower attachments were installed, in addition to 0.10 IPR where necessary. The plates were installed and the replacement protocol established every 15 days.
After finishing the use of the plates, the attachments were removed and the patient was scanned to make retainer plates. The treatment lasted 9 months until the patient entered the retention phase. The effectiveness of the combination of traditional and digital orthodontic techniques provided satisfactory results in a short period of time.
Fig 1(A-C) Initial extraoral photos
Fig 2 (A-E) Initial intraoral photos
Fig 3 Initial Cephalometry
Fig 4 Initial Teleradiography
Fig 5 Initial Overview
Fig 6 (A-C) Mini orthodontic implants in the infrazygomatic crest region and esthetic buttons and Elink type elastics
Fig 7 Strength measurement with a calibrated dynamometer
Fig 8 (A-B) 3D-BOT device installed
Fig 9 (A-E) Finishing with the use of aligners
Fig 10 (A-C) Final extra-oral photos
Fig 11 (A-E) Final intraoral photos
Fig 12 Final teleradiography
Fig 13 Final overview
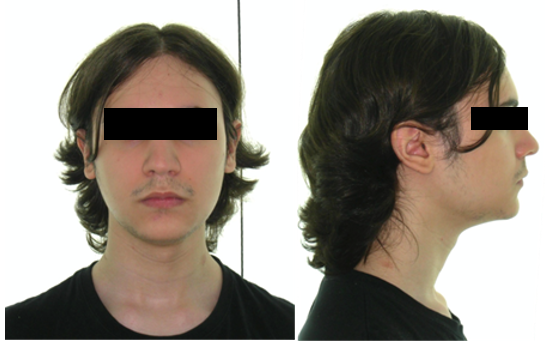

Fig 1 (A-C) Initial extraoral photos

Fig 2 (A-E) Initial intraoral photos
Fig 3. Initial Cephalometry
| SNA | 84° |
| SNB | 81° |
| ANB | 3.7° |
| Sn Go Me | 22° |
| FMA | 17° |
| IMPA | 106° |
| 1.PP | 123° |
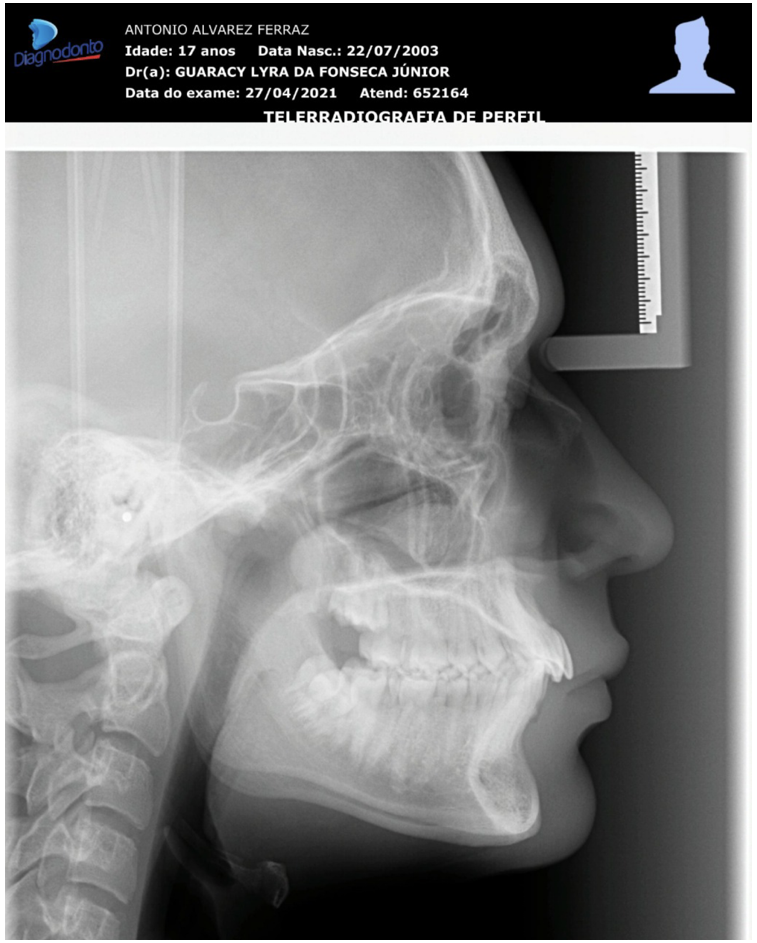

Fig 4- Initial Teleradiography Fig 5- Initial Overview

Fig 6- (A-C) Mini orthodontic implants in the infrazygomatic crest region and esthetic buttons and Elink type elastics

Fig 7 Strength measurement with a calibrated dynamometer
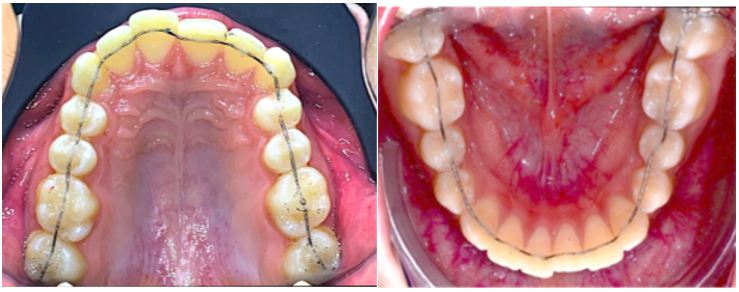
Fig 8 (A-B) 3D-BOT device installed




Fig 9 (A-E) Finishing with the use of aligners

Fig 10 (A-C) Final extra-oral photos

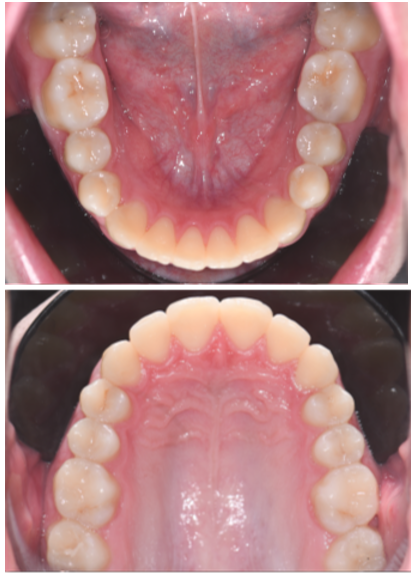
Fig 11 (A-E) Final intraoral photos
Fig 12 Final cephalometric analysis
| SNA | 81.45 |
| SNB | 79.83 |
| ANB | 1.62 |
| Sn Go Me | 25.34 |
| FMA | 19.15 |
| IMPA | 108.79 |
| 1.PP | 117.23 |

Fig 13: Final teleradiography

Fig 14: Final overview

Fig 15:Overlaying traces
DISCUSSION
The information obtained through the anamnesis and radiographic examinations was essential for choosing the treatment to be administered. Class II malocclusion, when amenable to orthodontic correction through dental compensation, presented an excellent response to treatment with the 3DBOT technique (Brackless orthodontics treatments), in association with maximum anchorage devices.6,8
This approach stands out for being comfortable and imperceptible, using a wire that passes through the palatal region of the anterior teeth and the occlusal region of the posterior teeth, thus meeting the esthetic demands frequently sought by patients. 9,10
Musilli (2008)11 reported that the BFO technique (Brackless fixed orthodontics) offers several differentials, such as root movement, non-interference in the patient’s phonetics and ease of cleaning, in addition to presenting a low load/deflection formality. These aspects are crucial to guarantee an effective and comfortable treatment.
The use of NEMOCAST software allowed the simulation of Class II malocclusion correction, as well as the desired dental position. With this tool, it was possible to measure the discrepancy and obtain models for the wire diagramming, contributing to a more predictable treatment.
Orthodontic mini-implants have proven to be an excellent option for temporary anchorage since they do not depend on patient cooperation and allow greater control over tooth movements, resulting in a significant reduction in treatment time. Although the extraction of two premolars is an acceptable approach in similar cases, it was decided to treat this case exclusively with distalization of the upper molars. 12,13,14,15,16,17
Lima Neto (2022)7 highlighted that the innovation of this approach is due to the insertion of mini screws in extra-alveolar locations, such as the infrazygomatic crest of the maxilla and the buccal shelf region of the mandible. This strategy allows greater autonomy in tooth movements since the position of the mini screws minimizes interference in the roots during tooth displacement.
Finishing treatment with clear aligners has proven to be an efficient and discreet choice, especially when combined with the aforementioned techniques. Technology also played a key role in planning and acquiring files for printing models and making the plates. Both bubble-type aligners and in-office digital aligners have their own advantages and challenges in orthodontic finishing and relapse treatment.18 ,19,20
All treatment was performed based on a virtual plan previously prepared by the orthodontist. In addition, Dolphin software was used for surgical planning, allowing for the overlapping of the profile teleradiography and the tracing, which enabled a detailed evaluation of the initial and final relationships of the molars.
In short, the combination of advanced orthodontic techniques and the use of innovative technologies demonstrate a commitment to effectiveness and esthetics in the treatment of malocclusions, providing satisfactory and predictable results for patients.
CONCLUSION
- The 3Dbot technique, in association with mini-implants and orthodontic aligners, has proven to be highly effective in correcting Class II malocclusion. The use of advanced technologies and specialized software has not only optimized the treatment approach, but has also contributed to significantly reducing the time required for its completion.
- Furthermore, this technique met the esthetic demands of patients, providing discreet and satisfactory orthodontic treatment. The results obtained indicate that the hybrid approach not only improved treatment efficiency, but also resulted in a considerable decrease in total treatment time.
- These findings highlight the relevance and innovation of the 3Dbot technique in contemporary orthodontics, demonstrating its potential to transform clinical practice.
REFERENCES
1 Lima AL, Valle CV, Tanaka OM. Variáveis relacionadas ao tratamento da má oclusão de Classe II: uma revisão sistemática. Dental Press J Orthod. 2009;14(5):41-9. doi:10.1590/S2176-94512009000500007. Disponível em: https://www.scielo.br/j/dpress/a/rW7YDNs4n7qdz3z95n76L3z/. Acesso em: 19 nov. 2024.
2 Fonseca J. Planejamento virtual no tratamento de más oclusões. Rev Bras Ortod. 2023.
3 Souza LT, Melo FJ, Andrade VM. Correção da Classe II sem extrações: uma revisão de literatura. Rev Ortod Estet. 2021;15(4):233-40. Disponível em: https://jmd.emnuvens.com.br/jmd/article/view/816. Acesso em: 19 nov. 2024.
4 Oliveira TR, Santos MA. Eficácia e limitações dos alinhadores estéticos na ortodontia. J Ortod Clin. 2019;17(2):45-52.
5 Silva LG, Oliveira RT. Técnicas ortodônticas estéticas e sua aplicabilidade na correção de más-oclusões de Classe II. J Bras Ortod. 2020;22(1):56-63.
6 Fonseca G, Tavares N, Freire CNBM, de Andrade EP, Gurgel G, Miguel A. Ortodontia estética, ancoragem esquelética em casos cirúrgicos ortognáticos. Orthod Sci Pract. 2022;15(59):19-26. doi:10.24077/2022;1559-220509.
7 Lima Neto ET, Fonseca Junior G, Cavalcante GRG, Gonçalves LR. Tratamento híbrido sem bráquetes da Classe II com auxílio de mini-implante extra-alveolar, distalizador versátil – relato de caso. Orthod Sci Pract. 2022;15(58):13-8.
8 Ferreira AP, Souza ME, Rocha TR. Correção de Classe II com técnicas de ancoragem máxima: uma revisão. Rev Ortod Estet. 2021;15(4):233-40.
9 Silva JM, Costa LF, Almeida RC. Aparelhos linguais: uma revisão sobre conforto e estética no tratamento ortodôntico. Rev Bras Ortod. 2020;25(3):102-10.
10 Fonseca Jr GL, Tavares N, Cavalcante GRG, Fonseca CH. Técnica ortodôntica fixa sem bráquetes, com tecnologia tridimensional “3D-BOT”. Orthod Sci Pract. 2019;12(46):22-30. doi:10.24077/2019;1246-2230.
11 Musilli M. The Bracketless Fixed Orthodontics: nine years of clinical experimentation. Prog Orthod. 2008;9(1):72-92.
12 Silva AB, Oliveira MC. Mini implantes como alternativa de ancoragem na ortodontia moderna. Rev Bras Odontol. 2018;25(2):125-32.
13 Costa RP, Lima TF, Santos EC. Distalização de molares em tratamentos de Classe II sem extrações: uma abordagem com mini implantes. J Ortod Clin. 2019;30(4):45-51.
14 Fonseca Junior G, da Silva Junior AM, Lima Neto NT, Lessa GRG, Betânia K, de Oliveira NAB. Tratamento objetivo de mordida aberta anterior utilizando Invisalign® e ancoragem esquelética – relato de caso. Orthod. Sci. Pract. 2023; 16(63):16-24.DOI: 10.24077/2023;1663-02236681495
15 Fonseca Júnior GL, Lima Neto NT, Lessa GRG, Brasileiro CB, Oliveira NAB, Farias KBM. Tratamento ortodôntico estético da má oclusão de Classe II com ancoragem esquelética: relato de caso. Ciênc Saúde. 2024;28(134):xx-xx. doi:10.5281/zenodo.11351317.
16 Fonseca Jr GL, et al. Tratamento compensatório da Classe III – ortodontia lingual e ancoragem esquelética: relato de caso. Revista Clínica de Ortodontia Dental Press. 2020;19(3):85-94.
17 Fonseca Jr GL, et al. Tratamento da Classe III com protração e retração em massa utilizando ancoragem esquelética. Orthodontic Science and Practice. 2020;13(50):39-46.
18 Lima Neto NT, da Fonseca Junior GL, Ribeiro CHD, Cavalcante GRG, de Melo MEC, Siqueira LF. Alinhadores ortodônticos para finalização de tratamentos ortodônticos e recidiva – relato de caso. Orthod Sci Pract. 2024;17(65):18-26. doi:10.24077/2024;17655878136234
19 Fonseca Junior GL, et al. Effect of the bracketless orthodontics technique and resin composite material on the biomechanical response of the upper central incisor: 3D finite element analysis. APOS Trends in Orthodontics, 2021.
20 Guaracy Lyra da Fonseca Junior et al. / Current Research in Dentistry 2021, Volume 12: 48.61 DOI: 10.3844/crdsp.2021.48.61
1-PhD in Orthodontics, Master in Orthodontics, SL Mandic-SP, Specialist in Orthodontics and Facial Orthopedics from the Paulista Society of Orthodontics SPO-SP, Professor and Coordinator of the Specialization Courses in Orthodontics – FACSETE-PE
2- Specialist in Orthodontics (CPGO-PE)
3- PhD in Orthodontics – SL Mandic-SP, Master in Orthodontics – SL Mandic-SP, Specialist in Orthodontics from the FACSETE-PE, Professor and Coordinator of the Specialization Courses in Orthodontics – FACSETE-RN,CPGO Recife.
4-Specialist in Orthodontics, Master and PhD in Orthodontics, Professor of the Specialization Course in Pediatric Dentistry – FACSETE-RN
5- Specialist in Orthodontics-FACSETE, CPGO Recife. Master in Orthodontics SL Mandic- SP, Professor of the Specialization Course in Orthodontics – FACSETE-CPGO Recife.
6- Specialist in Orthodontics and Master in Orthodontics – Uniararas – SP, Professor of the Specialization Course in Orthodontics – FACSETE-CPGO Recife.