REGISTRO DOI: 10.69849/revistaft/dt10202503161840
André Everton de Freitas1; Lindsay Rodrigues Salomé2; Nathalia de Freitas Silva2; Mérian Gomes França de Sousa2; Danilo Zorzam Santos2; Bianca Cecília de Jesus Cardoso2; Diego Braz da Silva2; Gisele Bailich3; Paulo Roberto Santos Lopes4; Marcelo de Carvalho Amorim5; Patrícia Roberta dos Santos6; Carolina Oliveira de Ávila7; Warley de Melo Oliveira8; Gustavo Heluy Damazio9
ABSTRACT
Background: To evaluate the evolution of patients with intra-articular fracture of the calcaneus submitted to surgical treatment. Methods: This observational, prospective cohort study included patients aged 18-65 years with intra-articular calcaneal fractures treated surgically using the lateral approach technique and blocked calcaneal plaque. Image exams assessed Bohler and Gissane angles and joint congruence. Physical examinations measured ankle joint range of motion (ROM) and utilized the AOFAS and FAOS scales. Data were collected 2 and 6 months postoperatively. Results: Sixteen patients with a mean age of 45.2 years participated. Average Gissane and Bohler angles were 127.2 ± 10.9 and 24 ± 13.9, respectively. The AOFAS questionnaire score was 43.69 ± 17.59. FAOS scores for pain, other symptoms, daily living activity, sports and recreation, and quality of life were 15.69 ± 9.99; 10.56 ± 4.80; 25.00 ± 15.91; 13.63 ± 6.09; and 8.88 ± 4.82, respectively. A positive correlation was found between AOFAS total score and dorsiflexion (rs = 0.526; p = 0.036). Conclusions: Adequate dorsiflexion range of motion is related to higher AOFAS scores, and an inverse correlation exists between Bohler’s angle and pain, daily life activity, and other FAOS symptoms.
Keywords: calcaneus, fracture, intra-articular, surgical, Bohler angle, Gissane angle, range of motion, AOFAS, FAOS.
INTRODUCTION
Axial load traumas in men aged 30 to 60 years represent a mechanism for calcaneal fractures, accounting for 1 to 2% of all fractures in general. (1) Such injuries are severe and typically occur after a fall from height or as a result of a traffic incident. Their incidence is higher in developing countries than in developed ones, and until 1990, there was no consensus on the appropriate approach for this type of fracture.(2,3)
Still in the 1990s, Sanders (5) had already demonstrated the importance of computed tomography as a predictor of the functional clinical outcome for patients with calcaneal fractures, influencing therapeutic choice and planning. However, postoperative evaluation of calcaneal fractures through tomography is still not a consensus, despite appearing to be a good indicator of the patient’s functional outcome.
Severe injuries, such as calcaneal fractures, are characterized by displaced fractures, including involvement of the articular surfaces, particularly affecting the subtalar joint. In cases of fragmented fractures, conservative treatment is chosen, allowing the fractured fragments to consolidate. Recovery in this case is prolonged, typically taking two years. However, the calcaneus remains deformed, the articular surfaces become incongruent, and limb alignment at the subtalar joint is lost. This may lead to osteoarthritis, chronic pain in the subtalar joint, and deformity in the affected foot.(2)
Calcaneal fractures hold significant socio-economic importance, as 20% of patients affected by this type of fracture are unable to return to work completely for up to three to five years after the injury.(4) This is crucial in developed countries due to the high health and social costs. In developing countries, the loss of economic potential has substantial implications for patients and their families. Additionally, patients with this type of fracture remain in the hospital for an extended period, incurring public expenses and benefiting from disability benefits for a prolonged duration.(2)
In the 1990s, computed tomography allowed for a better understanding of fracture patterns, leading to the development of new surgical approaches. This enabled improved reduction of bone fragments by stabilizing them with plates and screws, restoring the subtalar joint.(5) Observational studies of this treatment reported lower complication rates and better clinical outcomes than those observed in historical series of conservative treatment. This new approach to calcaneal fractures quickly spread in Europe, the United States, Canada, and Australia, and is now being implemented in developing countries as well.(6)
Gougoulias et al (2009), after evaluating general health indicators, injury scores, and radiographic parameters, expressed uncertainty about whether these parameters were better in post-surgical patients or those who underwent conservative treatment. These authors also questioned the benefits of surgery and its associated risks, concluding that more large-scale, carefully designed trials comparing surgical and non-surgical treatment are needed. Supporting this, Ågren et al (2013) showed that the benefits of surgical treatment were not superior to those of conservative treatment for intra-articular calcaneal fractures with displacement one year post-trauma. However, there appear to be some benefits at eight to twelve years, along with a lower prevalence of post-traumatic arthritis when evaluating radiographs. Nevertheless, radiographic findings alone seem insufficient to determine the patient’s functional outcome.(9)
The choice of treatment for calcaneal fractures remains a point of debate in orthopedics, and by correlating radiological findings with patient functionality, we aim to contribute more information to the selection of the best treatment for intra-articular calcaneal fractures.
Given the importance of appropriate treatment for articular fractures, the limited number of studies on calcaneal fractures treatment, and the lack of consensus on the preferred treatment for variations of these fractures, we selected intra-articular calcaneal fractures for this comparative functional evaluation of clinical and radiographic results. This choice is justified by the frequent complications, such as limitations and pain. By comparing with imaging studies, our objective is to correlate possible radiographic changes and preoperative patterns with specific patient complaints and certain complications. This may contribute to potential improvements in surgical treatment, therapeutic choice, and postoperative physiotherapeutic direction for calcaneal articular fractures.
The objective of this study was to evaluate the functionality of patients undergoing surgical treatment for intra-articular calcaneal fractures using the American Orthopaedic Foot and Ankle Society’s (AOFAS) 10 and Foot and Ankle Outcome Score (FAOS) 11 scales and to correlate the Bohler and Gissane angles with patient functionality through the AOFAS and FAOS scales.
METHODS
This is an observational cohort study conducted with patients with intra-articular calcaneal fractures undergoing surgical treatment at Maria Amélia Lins Hospital (HMAL) in Belo Horizonte, Minas Gerais, in 2018. Inclusion criteria: Patients aged 18 to 65 with intra-articular calcaneal fractures undergoing surgical treatment by the ankle and foot surgery team at HMAL using the same surgical approach (lateral access) and synthesis material (calcaneal locked plate). Exclusion criteria: Patients treated conservatively with plaster, those undergoing surgical treatment only with a cannulated screw, patients with psychiatric disorders, and those with another associated fracture were excluded.
The convenience sample consisted of 16 patients with intra-articular calcaneal fractures undergoing surgical treatment by the ankle and foot surgical orthopedic team at HMAL in 2018. Data collection for eligible patients was conducted in one stage after a minimum postoperative period of 2 months. The evaluation included radiographic imaging of the calcaneus in AP and axial views with load to determine the Bohler angle, Gissane angle, and post-surgical reduction articular congruence; three measures of ankle joint range of motion, considering the average value of the measurements; and the application of the AOFAS and FAOS questionnaires for clinical and functional evaluation of the ankle joint.
For better and proper study control, manuals containing each aspect of the protocol were produced and distributed to the study participants, along with training related to all research procedures and conduct. All activities in this study were carried out by trained health professionals for data collection and analysis. The data screening integrity was regularly monitored in a pre-prepared table containing omission and error data. Results were entered twice, and the origin of any inconsistent data was explored and resolved by the researchers. After the end of the planned data collection, the data were organized in an Excel spreadsheet and then transferred to the software used for statistical analysis (SPSS version 20.0). This study was submitted to the COEP of HMAL for research project approval. The ethical principles of research, as per the CNS regulation 466/12 on research involving human subjects, were ensured. The study posed no risks or harm to the studied population, as it analyzed results from imaging exams previously requested by the postoperative medical follow-up team.
Data were described using absolute frequencies and percentages for qualitative variables, mean and standard deviation for quantitative variables with normal distribution, otherwise described by median and (1st quartile; 3rd quartile). The Shapiro-Wilk test was used for normality. Pearson and Spearman correlation tests were conducted to analyze the correlation between radiographic findings and AOFAS and FAOS scales. Paired T-tests and/or Wilcoxon tests were used to assess Gissane and Bohler angles and ankle range of motion measures. The significance level was set at p<0.05, and the software used was SPSS version 20.0.
RESULTS
A total of 16 patients participated in the study, with an average age of 45.2 years (±14.4). Regarding gender, 37.5% were female, and 62.5% were male. Of these, 75% of the study patients had an incomplete first-year education, and 62.6% considered their health to be good or very good. Concerning the affected limb, 7 patients had the right lower limb affected, 7 the left, and 2 patients presented bilateral involvement. The observed trauma mechanisms were a fall from their own height in 93.8% (n=15) of cases and a motorcycle accident in 6.3% (n=1) (Table 1). The median postoperative time was 27.5 months (6.3; 67.5). The dorsiflexion range of motion had a median of 14º (7º; 17º), and the plantar flexion had an average value of 27.1º±14.3. For the Gissane and Bohler angles, the averages were 127.2º±10.9 and 24º±13.9, respectively. Table 2 presents the results of the AOFAS and FAOS scales. For the AOFAS questionnaire, an average score of 43.69 ±17.59 was observed. In the FAOS questionnaire, scores for the pain, other symptoms, activities of daily living, sports and recreations, and ankle and foot-related quality of life subscales had average values of 15.69±9.99, 10.56±4.80, 25.00±15.91, 13.63±6.09, and 8.88±4.82, respectively.
Table 1 – Results of the study’s quantitative variables
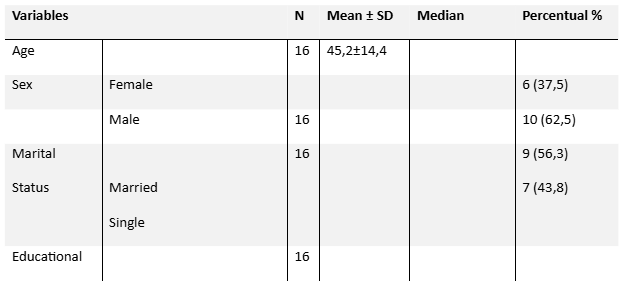
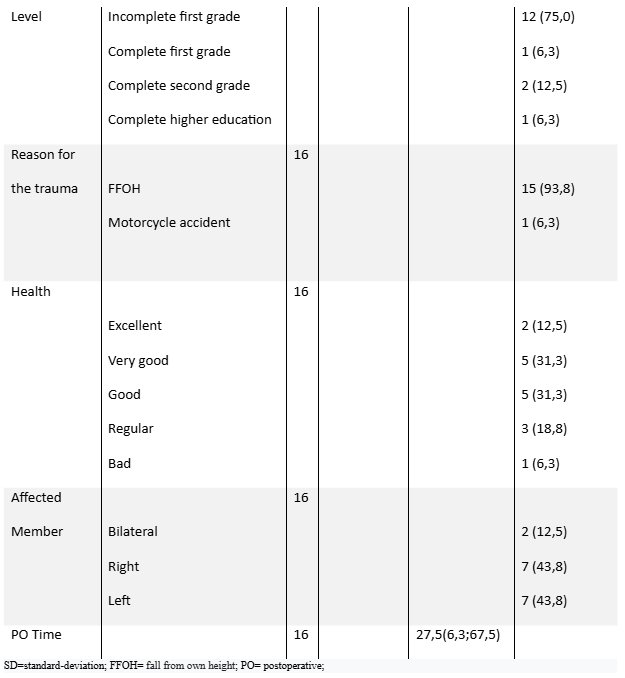
Table 2 – Results in the scale of life quality QVD and AOFAS
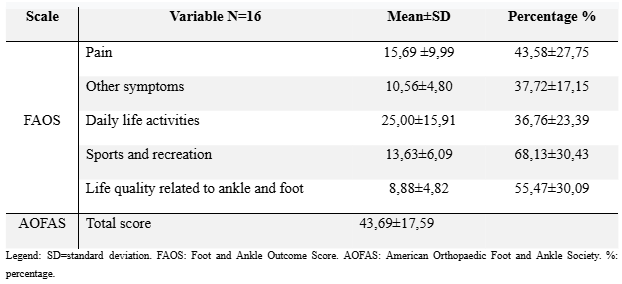
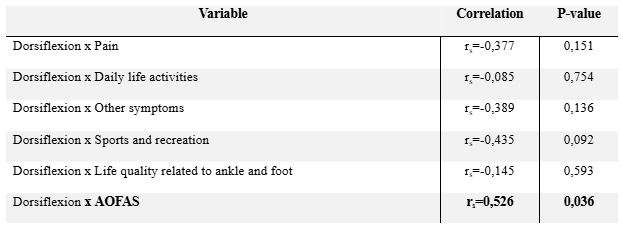
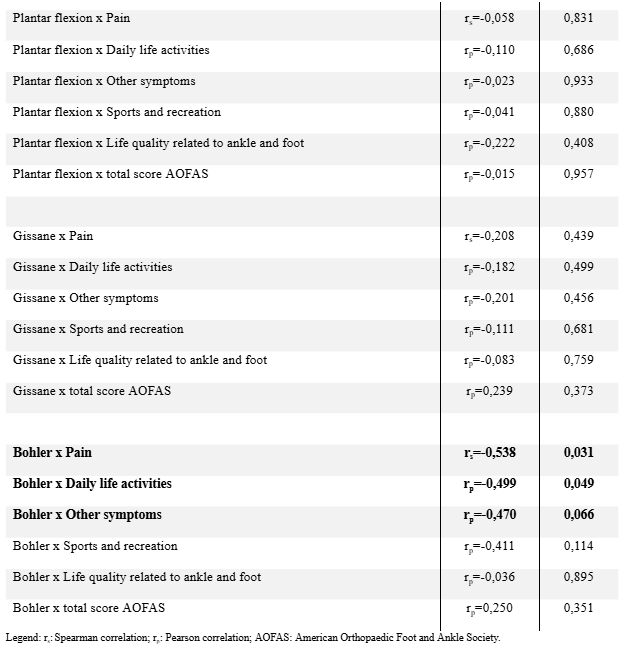
In Table 3, correlation analyses between study variables—dorsiflexion, plantar flexion, Gissane angles, Bohler angle—with AOFAS and FAOS scales were conducted. The significance level was set at p<0.05. A negative correlation was observed in the variables: pain (rs= -0.538; p=0.031) and activities of daily living (rp= -0.499; p=0.049) for the Bohler angle, and a positive correlation in the total AOFAS score for dorsiflexion (rs=0.526; p=0.036).
Table 3 – Results of the correlations between the life quality scales and the dorsiflexion, plantar flexion, Gissane and Bohler variables.
DISCUSSION
This study evaluated functionality through the AOFAS and FAOS scales and their correlation with Bohler and Gissane angles in patients with intra-articular calcaneal fractures undergoing surgical treatment. The results demonstrated dorsiflexion ranges of 14º (median) and plantar flexion of 27.1º (mean), sufficient for an adequate gait pattern development, where around 10º of dorsiflexion (DF) and 20º of plantar flexion (PF) are typically required. However, it is worth noting that, besides satisfactory joint mobility, other intrinsic factors such as muscle activation pattern, proprioception, and motor control are necessary for proper functionality, as well as postoperative pain. These aspects are reflected in the FAOS questionnaire’s subscale results, where the average values for pain, other symptoms, activities of daily living, sports and recreations, and ankle and foot-related quality of life accounted for 43.58%, 37.72%, 36.76%, 68.13%, and 55.47% of each subscale’s total value, respectively. For the AOFAS questionnaire, the mean score was 43.69±17.59. As the authors of these questionnaires chose not to relate numerical values to excellent, good, fair, and poor, it is observed in this study that the results for both questionnaires averaged below 50%, indicating unsatisfactory functionality despite an average range of motion for DF and PF.
In the correlation analyses conducted in this study, only a positive correlation was observed between DF range and the total score of the AOFAS scale, indicating that an increase in the DF angle corresponds to an increase in the total AOFAS score. Additionally, a negative correlation was observed between the Bohler angle and the pain, activities of daily living, and other symptoms sub-scales of the FAOS questionnaire. In other words, for each increase or decrease in the Bohler angle value, there would be an inversely proportional variation in the scores of these sub-scales. Considering that a decrease in the Bohler angle is expected in intra-articular calcaneal fractures, and knowing that one of the goals of surgical treatment is anatomical joint reduction and consequently the restoration of the Bohler angle, this study demonstrated that the postoperative increase, or restoration, of the Bohler angle is associated with a decrease in the pain, other symptoms, and difficulty in daily activities sub-scales of the FAOS questionnaire. Studies suggest improved functionality in patients undergoing surgical treatment with the restoration of the Bohler angle, but due to heterogeneity regarding fracture classification and treatment used, this correlation is not yet clear in the literature. Digenman et al (2017) observed statistically significant postoperative maintenance of Bohler, Gissane, and calcaneal varus angles, but they did not evaluate their correlation with functionality. Godos et al (2015), in a study with 153 surgically treated calcaneal fractures, suggested that Bohler angle restoration is necessary to achieve good functional outcomes and that poor outcomes were related to inadequate restoration of this angle. Other authors also suggest that postoperative Bohler angle restoration is related to better functional outcomes. (16,17,18)
Intra-articular calcaneal fractures remain a challenge for orthopedic surgeons, with many believing that anatomical restoration of the articular surface and stable fracture fixation are related to favorable outcomes. However, many aspects remain controversial, such as the type of surgical approach, technique used, evaluation methods, infections, postoperative complications, and rehabilitation. This study has limitations, including a small sample size and the omission of other variables that may interfere with patient functionality.
CONCLUSION
In conclusion, this study suggests that adequate dorsiflexion range is related to higher AOFAS scores, and an inversely proportional correlation was observed between the Bohler angle and pain, activities of daily living, and other symptoms of the FAOS scale. Further studies should be conducted to evaluate possible variables that may be related to the functionality of patients with surgically treated intra-articular calcaneal fractures.
CONFLICT OF INTEREST
The authors declare there is no conflict of interest.
ACKNOWLEDGMENTS
We extend our heartfelt thanks to the employees of Maria Amelia Lins Hospital for their unwavering support and assistance throughout this study. Their dedication and commitment were instrumental in the successful completion of this research.
FUNDING
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
REFERENCES
- Daftary A, Haims AH, Baumgaertner MR. Fractures of the calcaneus: a review with emphasis on CT. Radiographics. 2005 Sep-Oct;25(5):1215-26. https://doi.org/10.1148/rg.255045719
- Griffin D. Operative versus non-operative treatment for closed, displaced, intra-articular fractures of the calcaneus: randomised controlled trial. BMJ. 2014;349. https://doi.org/10.1136/bmj.g4483
- Bruce J, Sutherland A. Surgical versus conservative interventions for displaced intra-articular calcaneal fractures. Cochrane review [with consumer summary]. Cochrane Database of Systematic Reviews. 2013; Issue 1. https://doi.org/10.1002/14651858.CD000962.pub3
- Gülabi D, Sari F, Şen C, Coşkun C, Sağlam F, Erdem F, Bulut G. Mid-term results of calcaneal plating for displaced intraarticular calcaneus fractures. Ulus Travma Acil Cerrahi Derg. 2013;19(2):145-151. https://doi.org/10.5505/tjtes.2013.25796
- Sanders R. Intra-articular fractures of the calcaneus: present state of the art. J Orthop Trauma. 1992;6:252-265. https://doi.org/10.1097/00005131-199206000-00002
- Jain S, Jain AK, Kumar I. Outcome of open reduction and internal fixation of intraarticular calcaneal fracture fixed with locking calcaneal plate. Chin J Traumatol. 2013;16:355-60. https://doi.org/10.3760/cma.j.issn.1008-1275.2013.06.006
- Gougoulias N, Khanna A, McBride DJ, Maffulli N. Management of calcaneal fractures: systematic review of randomized trials. British Medical Bulletin. 2009;92:153–167. https://doi.org/10.1093/bmb/ldp008
- Ågren H, Wretenberg P, Sayed-Noor AS. Operative Versus Nonoperative Treatment of Displaced Intra-Articular Calcaneal Fractures, A Prospective, Randomized, Controlled Multicenter Trial. J Bone Joint Surg Am. 2013 Aug 07;95(15):1351-1357. https://doi.org/10.2106/JBJS.L.00740
- Schepers T, Ginai AZ, Mulder PGH, Patka P. Radiographic evaluation of calcaneal fractures: to measure or not to measure. Skeletal Radiol. 2007;36:847–852. https://doi.org/10.1007/s00256-007-0297-1
- Rodrigues RC, et al. Tradução, adaptação cultural e validação do “American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot Scale”. Acta ortop. bras. [online]. 2008;16(2):107-111. https://doi.org/10.1590/S1413-78522008000200004
- Imoto AM, Peccin MS, Rodrigues R, Mizusaki JM. Translation, cultural adaptation and validation of foot and ankle outcome score (FAOS) questionnaire into Portuguese. Acta Ortop Bras. [online]. 2009;17(4):232-5. https://doi.org/10.1590/S1413-78522009000400006
- Perry J. Gait Analysis, normal and pathological function. Thorofare, N. J: Slack; 1992.
- Cottom JM, Baker JS. Restoring the Anatomy of Calcaneal Fractures: A Simple Technique with Radiographic Review. Foot Ankle Specialist. 2016;9(2):145-152. https://doi.org/10.1177/1938640016636932
- Dingemans SA, Sintenie FW, Jong VM, Luitse JSK, Schepers T. Fixation Methods for Calcaneus Fractures: A Systematic Review of Biomechanical Studies Using Cadaver Specimens. The Journal of Foot & Ankle Surgery. 2017;56(3):479-485. https://doi.org/10.1053/j.jfas.2017.01.003
- Gołos J, Kwiatkowski K, Piekarczyk P, Cieślik P, Rowicki K, Waliński T. Long-term Results of Operative Treatment of Calcaneal Fractures. Traumatologia Rehabilitacja. 2015;17(2):163-174. https://doi.org/10.5604/15093492.1157190
- Makki D, Alnajjar HM, Walkay S, Ramkumar U, Watson AJ, Allen PW. Osteosynthesis of displaced intra-articular fractures of the calcaneum: a long-term review of 47 cases. J Bone Joint Surg Br. 2010;92:693–700. https://doi.org/10.1302/0301-620X.92B5.23036
- Su Y, Chen W, Zhang T, Wu X, Wu Z, Zhang Y. Bohler’s angle’s role in assessing the injury severity and functional outcome of internal fixation for displaced intra-articular calcaneal fractures: a retrospective study. BMC Surg. 2013;13:40. https://doi.org/10.1186/1471-2482-13-40
- Isaacs JD, Baba M, Huang P, Symes M. The diagnostic accuracy of Bohler’s angle in fractures of the calcaneus. J Emerg Med. 2013;45(6):879-84. https://doi.org/10.1016/j.jemermed.2013.05.036
- Griffin D, Parsons N, Shaw E, et al. Operative versus non-operative treatment for closed, displaced, intra-articular fractures of the calcaneus: randomised controlled trial. BMJ. 2014;349. https://doi.org/10.1136/bmj.g4483
- Zhang W, Lin F, Chen E, Xue D, Pan Z. Operative versus non-operative treatment of displaced intra-articular calcaneal fractures: a meta-analysis of randomized controlled trials. J Orthop Trauma. 2015;30 –81. https://doi.org/10.1097/BOT.0000000000000297
1Department of Orthopedics, Maria Amélia Lins Hospital, Belo Horizonte, Minas Gerais, Brazil, Email: aefreitas13@gmail.com
2Department of Physiotherapy, Faculdade Pitágoras, Belo Horizonte, Minas Gerais, Brazil, Email: lindsayrodrigues68@gmail.com; Email: Nathalia.freitassilva97@gmail.com; Email: fisiome17@gmail.com;
Email: danilozorzam@outlook.com; Email: bibicecilia@hotmail.com; Email: diegoobrazs@hotmail.com
3Department of Biology, Centro Universitário para o Desenvolvimento do Alto Vale do Ita- jaí, Santa Catarina, Brazil, Email: gisele.bailich@unidavi.edu.br
4Department of Physiotherapy, Centro Universitário para o Desenvolvimento do Alto Vale do Itajaí, Santa Catarina, Brazil, Email: pauloroberto@unidavi.edu.br
5Department of Orthopedics, Hospital Mater Dei, Belo Horizonte, Minas Gerais, Brazil, Email: marcelocamorim@yahoo.com.br
6Department of Medicine, Faculdade ZARNS, Itumbiara, Goiás, Brazil, Email: patriciarsantosgi@gmail.com
7Medical Student, Faculdade ZARNS, Itumbiara, Goiás, Brazil, Email: carolina.avila0504@gmail.com
8ACCESS Fisioterapia, Belo Horizonte, Minas Gerais, Brazil, Email: aefreitas13@gmail.com
9Department of Orthopedics, Maria Amélia Lins Hospital, Belo Horizonte, Minas Gerais, Brazil, Email: gdheluy@uai.com.br