REGISTRO DOI: 10.5281/zenodo.10615537
Rodrigo Gothe1
Marcelo Germani Vieira1
Lorena Toledo Alves1
Adriana Mendonça da Silva1
Viviane de Azevedo Rabelo1
Victor Rogério1
Natália Galvão Garcia2*
ABSTRACT
Botulinum toxin is a neurotoxin produced naturally by Clostridium botulinum bacteria. The use of botulinum toxin type-A (BTA) for rejuvenation and improvement of facial has thus been achieving positive results in the treatment of dynamic wrinkles, particularly in the upper facial structures such as glabellar lines, horizontal frontalis lines, periorbital lines, nasal lines, and an improvement of the positioning of the eyebrows. However, there is still no consensus in the scientific literature on the best approach for repositioning the eyebrows. Thus, the present study aims to report a clinical case using botulinum toxin for repositioning of eyebrows and rejuvenation of the upper third of the face. In total, 58 units of BTA were applied, distributed among the muscles of the upper third of the face to improve the eyebrow arch and to soften dynamic wrinkles, promoting facial rejuvenation. The patient reported satisfaction with the results, particularly with regard to the repositioning of the eyebrows. The botulinum toxin also provided satisfactory results in smoothing dynamic wrinkles, especially those in the frontalis and glabellar regions. Through the presentation of this clinical case, it is possible to state that the clinical protocol used for the application of botulinum toxin was effective in the repositioning of the eyebrows and rejuvenation of the upper third of the face.
Key words: Botulinum toxin, Face, Rejuvenation
INTRODUCTION
With the onset of aging, noticeable changes occur in the face. Loss of bone density and skin elasticity, along ith the onset of aging, noticeable changes occur in the with the hyperdynamic contraction of the muscles, cause tissues to follow in a descending motion, facilitating the formation of wrinkles that result in an aged appearance.[1-3] In the past decade, an increasing number of patients, concerned with the early signs of facial aging, have begun to seek minimally invasive esthetic procedures as botulinum toxin.[4,5]
Botulinum toxin is a neurotoxin produced naturally by Clostridium botulinum bacteria. Of the seven known serological toxins produced, type A is most often used as it is the most potent.[2] Developed in laboratories, botulinum toxin type-A (BTA) is available in crystalline form, stable, and lyophilized in human albumin and is commercialized vacuum dried in sterile vials that should be diluted in saline solution.[3] The three leading global brands of BTA are Botox/Vistabel (Allergan Inc., USA), Dysport (Ipsen Limited, UK), and Xeomin/Bocouture (Merz Pharmaceuticals GmbH, Germany).[4]
The use of BTA for rejuvenation and improvement of facial esthetics is made possible through its mechanism of action. This neurotoxin is able to reduce muscular activity through the inhibition of acetylcholine discharge of in the muscle junction, resulting in a reduction of hyperdermic lines and correction of facial asymmetry.[6,7] BTA has, thus, been achieving positive results[8] in the esthetic treatment of dynamic wrinkles, particularly in the upper facial structures such as glabellar lines, horizontal frontalis lines, periorbital lines, nasal lines, and an improvement of the positioning of the eyebrows.[9]
The use of botulinum toxin for the repositioning of the eyebrows is justified for both esthetic and functional reasons, as in addition to the sagging of the eyebrow contributing to a tired and aging look, the excessive eyelid skin can obstruct vision.[10] As such, the temporary paralyses of specific muscles in the upper third of the face result in an elevation of the eyebrows, giving patients back physical traits associated with youth and beauty. However, there is still no consensus in the scientific literature on the best approach for repositioning the eyebrows.[11] Thus, the present study aims to report a clinical case using botulinum toxin for repositioning of eyebrows and rejuvenation of the upper third of the face.
CASE REPORT
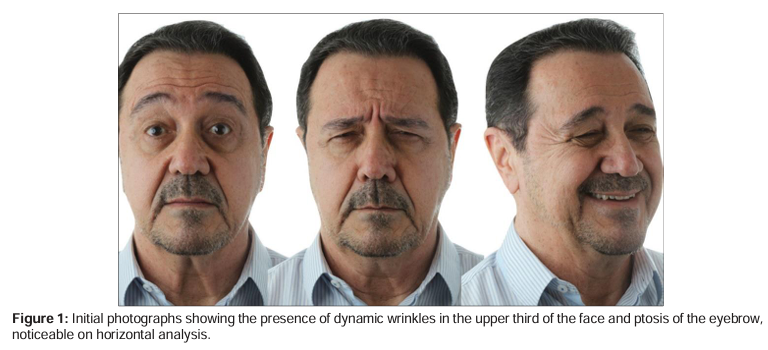
A male patient, age 74, came to the clinic and his main concern was a “sad” face. During the anamnesis, the patient reported never having undergone treatment with botulinum toxin. On clinical examination, initial photographs were taken [Figure 1] of the patient. To facilitate and guide the diagnosis, the photographs were taken with the facial mimic muscles at rest and in movement.
In light of the significant ptosis of the outer tip of the eyebrow observed through horizontal analysis of the upper third of the face [Figure 2], a conservative treatment approach was selected, concentrating application of BTA more in the glabellar region and less in the frontalis region. Five application sites were selected in the frontalis region with an injection of two units BTA per site, totaling 10 units in the frontalis muscle [Figure 3a]. In the glabellar region, application of an additional 22 units BTA was planned, with 2 units applied in each site [Figure 3b]. In total, three application sites were planned in the procerus muscle with an additional four sites in each brow bone corrugator muscle [Figure 3c].
For the treatment of the dynamic wrinkles in the upper third of the face, application of BTA was planned in the nasal region and in the orbital region of the eyes. Four units were injected, two in each site. In the orbital muscle of each eye, injection of 10 units BTA was planned, divided equitably among five sites. An injection of one unit BTA was applied in the orbital muscles of each eye, in the direction of the eyebrow arch, aiming to make the patient’s eyes look wider and to aid in the treatment of the eyebrow ptosis.
In total, 58 units BTA were applied, distributed among the muscles of the upper third of the face to improve the eyebrow arch and to soften dynamic wrinkles, promoting facial rejuvenation.
The botulinum toxin selected to treat this case was abobotulinum A (ABO; Dysport/Ipsen Limited, Slough Berkshire, UK) containing 500 European units. For the reconstitution, 2.5 ml saline solution to 500 units botulinum toxin was utilized, following the recommendations of the manufacturer.
Twenty-one days after treatment, the patient returned to the clinic for follow-up evaluation and to document the case. New photographs of the patient were taken for comparison and evaluation of the results of the eyebrow repositioning and smoothening of the wrinkles in the upper third of the face.
The patient reported satisfaction with the results, particularly with regard to the repositioning of the eyebrows [Figure 4a and b]. The botulinum toxin also provided satisfactory results in smoothing dynamic wrinkles, especially those in the frontalis [Figure 5a] and glabellar regions [Figure 5b] but produced less than satisfactory results in the orbital region [Figure 5c].
DISCUSSION
The determination of the best approach to correct eyebrow position requires an evaluation of some of its characteristics, such as degree and extension of the sagging, thickness of the eyebrow, presence of glabellar and frontalis wrinkles, and height of hair implantation.[11] The patient in question had eyebrow ptosis that was noticeable, but nevertheless considered mild according to the classification criteria,[6] without dermatochalasis (excessive eyelid skin), and with the presence of glabellar and frontalis wrinkles. An evaluation of these characteristics using facial analysis suggested that treatment with botulinum toxin was a viable approach for the case.
For the present reported case, we opted for a conservative approach with BTA. The fact that the patient is male determines a need to try to position the eyebrow closer to the level of the orbital edge, with a more discreet arch. A larger application of BTA could result in chronically surprised look
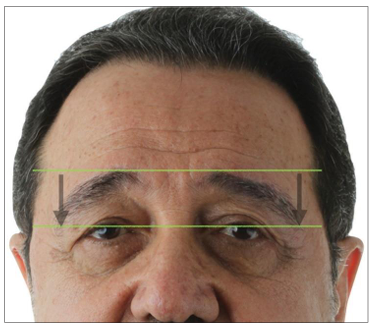
Figure 2: The eyebrow observed through horizontal analysis of the upper third of the face due to the exaggeration of the brows or of the medial portion, or in an angry look due to an increased elevation of the ends and a lower positioning of the middle.[3]
due to the exaggeration of the brows or of the medial portion, or in an angry look due to an increased elevation of the ends and a lower positioning of the middle.[3]
In addition, the patient had never undergone treatment with BTA before this visit. Application of BTA in a conservative manner would, therefore, allow for initiating with the lowest possible doses of the toxin and a follow-up of how the patient would respond to further evaluate the need to alter the proposed protocol, taking into account the individual characteristics of each patient’s face and the need for a tailored and progressive treatment. The use of smaller doses is initially advised as there is nothing definitive in the literature that reverses the process of muscle paralysis except the process formation of new motor plates that gradually activate the muscle overtime, usually within 3–6 months.[4,8]
During planning, it was determined that BTA would be applied in the frontalis and glabellar regions, but also in the nasal and orbital region of the eyes, for two reasons: First, because the eyebrow ptosis, which was the patient’s main concern, the patient had dynamic wrinkles around his nose and eyes and applying botulinum toxin in these areas allowed for a better result in regard to rejuvenation of the upper third of the face. Second, because studies[3,7] show that BTA in the upper third of the face should be applied in conjunction with the four regions (glabella, frontalis, and nasal orbital), so as to avoid an increased movement of the muscles that were not treated in this region.
There is an intense debate regarding the comparability of the different BTA formulations available on the market – onabotulinumtoxinA, incobotulinumtoxinA, and abobotulinumtoxinA – with regard to potency diffusion, pain on application sites, and duration of the effects.[8-11] These three formulations are chemically and pharmacologically unique, and their doses are not interchangeable. Despite these differences, a conversion value can be found between them, allowing their exchange in medical practice.[5,8] As for clinical efficacy, these formulations are similar when administered correctly, with ABO, approved under the brand name Dysport (Azzalure), being the cost effective.[3]
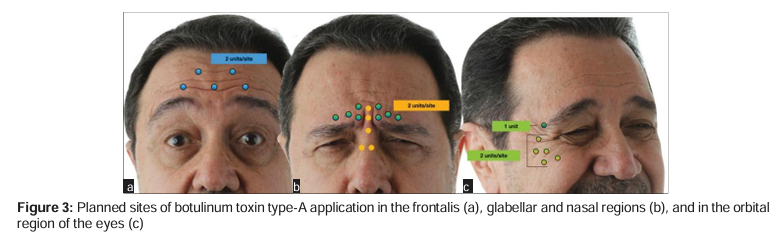

Figure 4: Position of the eyebrows before and after applying botulinum toxin, moving from an unsatisfactory position (a) to a more satisfactory arch (b)
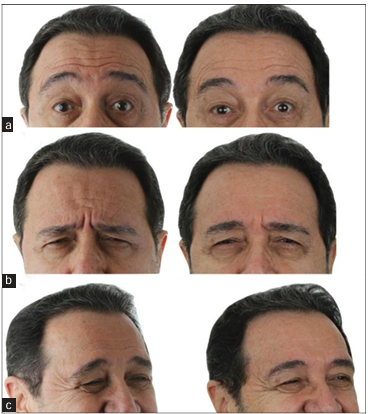
Figure 5: Photographs comparing before and after botulinum toxin application for the treatment of the dynamic wrinkles in the frontalis region (a), glabellar region (b), and orbital region of the eyes (c)
The results achieved with the treatment proposed were successful in achieving rejuvenation of the upper third of the face and met the patient’s expectations, who demonstrated satisfaction with the results achieved. The repositioning of the eyebrow was noticeable, greatly improving the patient’s main concern, and reduced the existing wrinkles in the frontalis and glabellar regions. With regard to the reduction of wrinkles in the orbital region, the desired result was not achieved. Considering that reapplications and touch-ups are not recommended before a period of 3 months due to the antigenic profile of the BTA and the likelihood of the formation of antibodies,[3] after this period of 3 months is over, an adjustment will be made, increasing the dose of BTA that will be applied, to reach more effective paralysis of the orbital eye muscle.
CONCLUSION
Through the presentation of this clinical case, it is possible to state that the clinical protocol used for the application of botulinum toxin was effective in the repositioning of the eyebrows and rejuvenation of the upper third of the face. Therefore, it is suggested that this protocol can assist other professionals in planning a similar treatment, always respecting the individuality and needs of each patient.
ETHICAL APPROVAL
A consent form for publication of the article was previously signed by the patient.
FUNDING INFORMATION
No funding received.
INFORMED CONSENT
Informed consent was obtained from all individual participants included in the study.
AUTHORS’ CONTRIBUTIONS
- Lorena Toledo Alves; Adriana Mendonça da Silva – have made substantial contributions to conception and acquisition of data.
- Victor Rogério; Viviane de Azevedo Rabelo – have made substantial contributions to carry out the treatment.
- Marcelo Germani Vieira – accountable for all aspects of the treatment.
- Natália Galvão Garcia – been involved in drafting the manuscript, revising it critically for important intellectual content.
- Rodrigo Cardoso Gothe – have made substantial contributions to conception and acquisition of data.
COMPETING OF INTERESTS
The authors declare no conflicts of interest.
REFERENCES
1. Wong CH, Mendelson B. Newer understanding of specific anatomic targets in the aging face as applied to injectables: Aging changes in the craniofacial skeleton and facial ligaments. Plast Reconstr Surg 2015;136:44S-8.
2. Lee TS, Wang L, Han R, Mourad M, Ducic Y. Options in repositioning the asymmetric brow from paralysis and trauma. Facial Plast Surg 2017;33:627-38.
3. Sundaram H, Signorini M, Liew S, de Almeida AR, Wu Y, Vieira Braz A, et al, Global Aesthetics Consensus Group. Global aesthetics consensus: Botulinum toxin Type A–evidence-based review, emerging concepts, and consensus recommendations for aesthetic use, including updates on complications. Plast Reconstr Surg 2016;137:518e-29.
4. Carruthers JD, Glogau RG, Blitzer A, Anderson RL, Cohen JL, Cox SE, et al. Advances in facial rejuvenation: Botulinum toxin Type A, hyaluronic acid dermal fillers, and combination therapies-consensus recommendations. Plast Reconstr Surg 2008;121:5-30.
5. Raspaldo H, Niforos FR, Gassia V, Dallara JM, Bellity P, Baspeyras M, et al. Lower-face and neck antiaging treatment and prevention using onabotulinumtoxin A: The 2010 multidisciplinary French consensus-Part 2. J Cosmet Dermatol 2011;10:131-49.
6. Kattimani V, Tiwari RV, Gufran K, Wasan B, Shilpa PH, Khader AA. Botulinum toxin application in facial esthetics and recent treatment indications (2013-2018). J Int Soc Prev Community Dent 2017;8:71-81.
7. Har-Shai Y, Gil T, Metanes I, Scheflan M. Brow lift for the correction of visual field impairment. Aesthetic Surg J 2008;28:512-7.
8. de Miranda RE, Matayoshu S. Procedimentos cirúrgicos e não cirúrgicos para elevação das sobrancelhas : Revisão sistemática e fluxograma de abordagem. Rev Bras Cir Plast 2019;34:539-45.
9. Yalçinkaya E, Cingi C, Söken H, Ulusoy S, Muluk NB. Aesthetic analysis of the ideal eyebrow shape and position. Eur Arch Otorhinolaryngol 2016;273:305-10.
10. Brennan C. Botulinum toxin Type-A (BoNT-A) injections of the corrugator muscles for aesthetics and depression? Plast Surg Nurs 2016;36:167-9.
11. Sattler G, Callander MJ, Grablowitz D, Walker T, Bee EK, Rzany B, et al. Noninferiority of incobotulinumtoxin a, free from complexing proteins, compared with another botulinum toxin Type A in the treatment of glabellar frown lines. Dermatol Surg 2010;36:2146-54.
How to cite this article: Vieira MG, Alves LT, da Silva AM, Rabelo VA, Rogério V, Garcia NG, GOTHE, R. C.
Botulinum Toxin for Eyebrow Repositioning and Facial Rejuvenation – case report. J Clin Res Dent 2020;3(1):1-5.
1Let`s Hof Academy, Sao Paulo, Sao Paulo, Brazil
2School of Dentistry, University Centre of Lavras, Minas Gerais, Brazil